Sexual health: Taking control
Pharmacy Magazine,
![]() 4 Min
4 Min
Pharmacy Magazine,
![]() 4 Min
4 Min
Pharmacy Magazine,
![]() 4 Min
4 Min
After reading this feature you should be able to:
The UK still has one of the highest teenage pregnancy rates in Europe, even though numbers have fallen markedly and were at an all-time low in 2012. Since 1998 the conception rate for under-18s has fallen by 41 per cent and in 2014 the total number of abortions in the under-18s was 11 per 1,000 women (down from 18 per 1,000 women in 2004). Forty-nine per cent of conceptions in under-18s result in abortion.
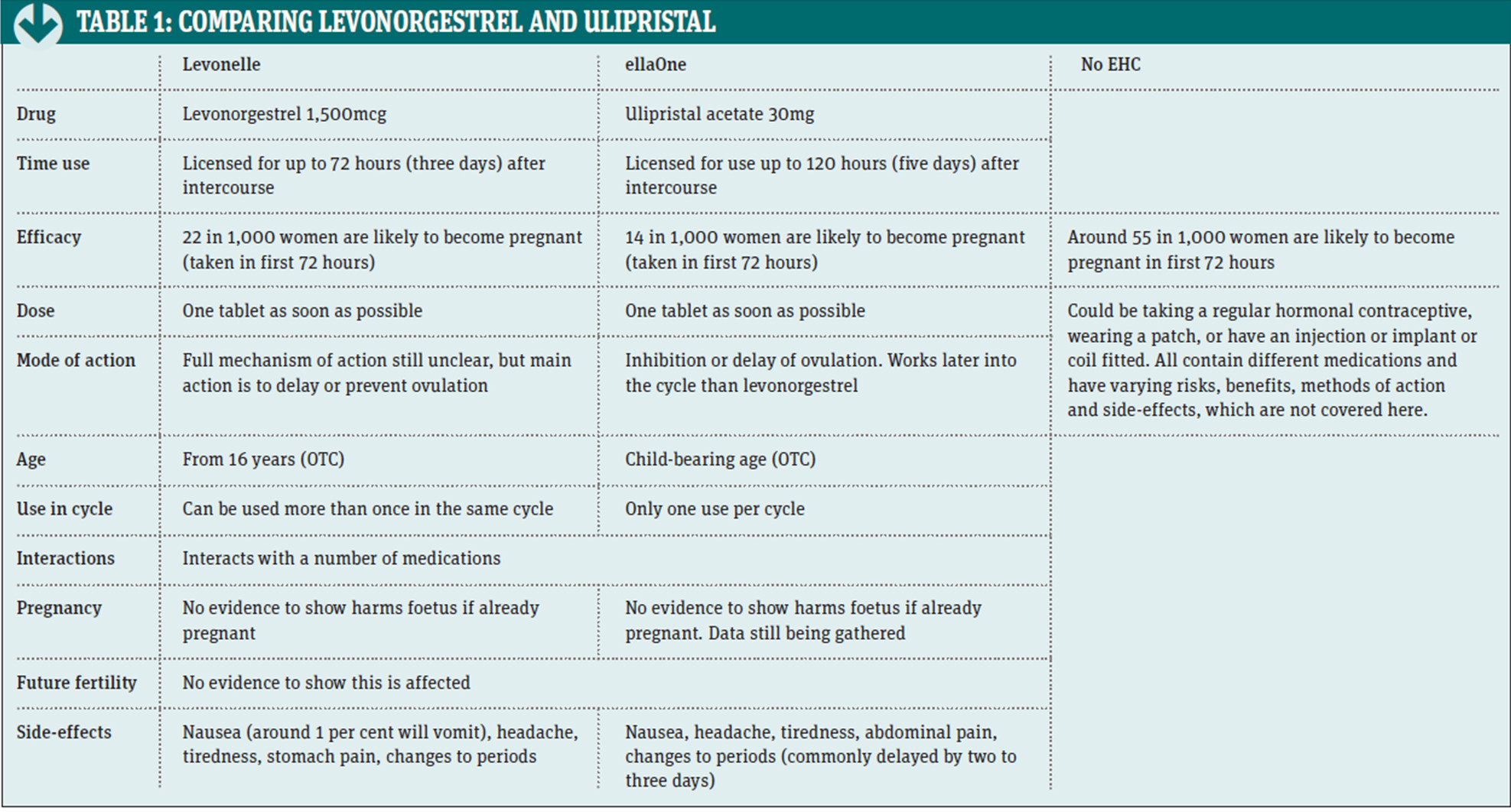
Ulipristal acetate (ellaOne) was launched earlier this year and is the first addition to the OTC emergency hormonal contraception category since levonorgestrel in 2001. There are a number of differences between ulipristal acetate and levonorgestrel, which are highlighted in Table 1 below.
Pharmacies have a number of advantages when it comes to providing both EHC and contraception advice compared to GPs and other formal clinic settings. Open outside usual clinic or GP hours, pharmacies can be accessed confidentially and without an appointment. Consultations also provide the opportunity to advise on sexually transmitted infections, both verbally and with written information.
Some areas have chlamydia testing schemes. Studies in NHS Southwark reported that 16 per cent of those tested in pharmacies for chlamydia would not have been screened elsewhere. One argument against OTC provision of EHC is that it could encourage increased risky sexual behaviour or increased EHC use rather than the use of regular contraception.
However, a UK-wide study shows that only 4 per cent of those involved received EHC more than twice in any year and 70 per cent started regular contraception within one year of receiving EHC. Interestingly, another study shows that most EHC supplies in pharmacies are carried out on a Sunday or Monday when other services are unavailable or obtaining appointments is more difficult.
Overall, increasing access to EHC via pharmacy has been shown to reduce the number of unwanted pregnancies. In City and Hackney, for example, the teenage pregnancy rate fell by 28 per cent over 10 years. Since then, pharmacies have continued to supply EHC, both as a POM and under PGDs, with evidence continuing to show that supply has helped to reduce pregnancy rates.
Sexual attitudes over the past 60 years have changed and a study from UCL shows that the average age of first intercourse has fallen to 16 years of age for both sexes from 19 years (women) and 18 years (men).
The average age of mothers is increasing, with ONS statistics showing that the average conception age has increased from 27.9 years in 1992 to 29.8 years in 2012, continuing the steady increase seen since 1976. NICE guidance highlights the need to ensure that €young women and young men have easy access to the full range of contraceptive methods€.
The 2013 Framework for Sexual Health Improvement in England also contains a key priority to reduce the number of unwanted pregnancies by increasing access to €all methods of contraception€. While the focus of the guidance is on pregnancy in young people, it is of course equally applicable to older women. For this group, the convenience of a community pharmacy with no appointment, open outside traditional working hours and with access to a full range of information and advice as well as EHC is extremely important.
Safeguarding issues have become much more important in recent years with the widening availability of EHC to young people, both OTC and via PGDs. Detecting abuse can be difficult in the pharmacy setting, but there are various signs to be aware of which may warrant further questioning of the client. These include:
The groups of children at increased risk of abuse include those:
It should be remembered that under-16s are under the age of consent. Two teenagers of similar age having a consensual sexual relationship is viewed as acceptable but it is an offence for anyone over 18 years to have any sexual activity with someone under 18 if the older person holds a position of trust.
Rape is committed by a man intentionally penetrating his penis into the mouth, anus or vagina of a person under 13 years, or without consent from anyone over this age. In an EHC consultation, all under-16s must be assessed for Gillick Competence.
Any abuse suspected in under-18s must be reported to the local safeguarding children's officer, so it is a good idea to have up-todate contact details of the local safeguarding children's team and safeguarding adults' team in the pharmacy. Pharmacists have a duty to refer suspected cases of neglect or abuse to social care or the police.
Concerns should be discussed with a named or designated healthcare professional and a record should be made of actions taken as a criminal investigation could follow. See: What to do if you're worried a child is being abused for more information.
There may be times when it is necessary to break the confidentiality of an EHC consultation. This should be discussed with the person concerned, unless there are significant reasons not to do so, such as increasing the risk to that person. The local safeguarding board can be contacted for advice without breaking confidentiality.
The Department of Education's €Information sharing: guidance for practitioners and managers€ lists seven 'golden rules' for information sharing, while the GPhC has a useful document entitled €Guidance on patient confidentiality€. If an area has a PGD for emergency contraception, it is likely that, as part of the terms, some sort of safeguarding training must be completed.
A good overall healthy diet, not smoking, a low alcohol intake and less stress will all help to promote fertility but recent studies have shown that other factors can be involved as well.
A small study presented at the European Congress of Rheumatology in June added to previous research that taking NSAIDs reduces the chances of becoming pregnant by preventing ovulation. The effect was most striking with diclofenac, with ovulation occurring in only 6.3 per cent of the participants who had taken the NSAID for 10 consecutive days, compared to 100 per cent of the control group.
The study also showed lower progesterone levels could prevent the implantation of a fertilised egg. Fertility levels returned to normal once the NSAID had been stopped. Further research is needed to determine more detail about the effects of the length of time and dose taken.
Studies have found that vitamin D can play a role in sperm and ovarian cells and could affect sex hormone levels. Removing the vitamin D receptor resulted in reduced sperm count and mobility, and changes to the ovarian and placental structure in mice. Another study showed changes to implantation varying between summer and winter.
In another study it was found that fertility could increase by as much as one-third in sunny weather, with improved rates of fertilisation, pregnancy and live births, as well as the quality of the eggs produced. This is thought to be due to increased melatonin levels €“ known to affect fertility. The increase in vitamin D is believed to improve the quality of the eggs produced.
Regular consumption of fruit, vegetables and pulses in both men and women is associated with greater fertility €“ thought to be due to the antioxidant content, and that less fatty food and red meat are likely to be eaten by those who eat more fruit and vegetables. Five-a-day is recommended for optimal fertility but this advice has been countered by other studies reporting that pesticides on fruits could be reducing fertility in men by affecting sperm count.
In one small study fertility was reported to be around 49 per cent lower between the highest and lowest consumers of fruit. Fruit and vegetables should be washed to remove surface pesticide residue.
To help customers locate the sexual wellbeing category in pharmacy with ease, Mark Pearson, Durex marketing director at RB, recommends positioning the category within the healthcare fixture, near family planning and female care products, as well as in secondary locations, such as at the check-out and next to male grooming products.
To aid navigation, he stresses the importance of 'brand-blocking' and positioning Durex, the signpost brand, at eye level. He also advises stocking a range of condoms, lubricants, gels and toys to support the needs of consumers of all ages and life-stages.
€RB research has proven that making the category easier to find unlocks impulse purchasing and also supports ease of find for those embarrassed about shopping the category,€ he says, adding that pharmacy teams have a strong role to play in helping to normalise the category. To improve their knowledge of the category, pharmacy teams can complete a sexual health module via RB's training portal.