
In Learning
Follow this topic
Bookmark
Record learning outcomes
Good bowel health is characterised by regular, comfortable digestion, minimal adverse symptoms and a healthy gut microbiome. As the functions of the gastrointestinal (GI) system are supported by organs including the liver, gallbladder, pancreas, small intestine, large intestine and rectum — and because these systems interact closely — symptoms can arise at any point along the GI tract.
Learning Objectives
After reading this feature you should be able to:
- Recognise common lower GI presentations encountered in community pharmacy – in particular, constipation and diarrhoea.
- Apply structured history-taking to distinguish self-limiting symptoms from red flags requiring referral.
- Recommend appropriate lifestyle, dietary and therapeutic options.
Gastrointestinal symptoms are very common. A recent survey of UK adults found that 86% had experienced GI symptoms in the previous month,1 with 91% describing this as their usual experience. The most reported symptoms were flatulence (72%), bloating (64%) and abdominal rumbling (58%).
When respondents were asked about more severe or worrying symptoms, the reporting dropped significantly. Bloating was reported by 18%, followed by abdominal pain (16%) and diarrhoea (13%). Notably, 72% stated that they did not have an existing GI condition.
As prescribing is restricted for some GI conditions, including infrequent constipation and adult diarrhoea, pharmacy teams have an important role in assessing and managing common lower GI presentations. This article focuses on how constipation and diarrhoea should be assessed and managed.
Key Facts
- Nearly nine out of 10 adults regularly report GI symptoms, with flatulence, bloating and abdominal rumbling among the most common.
- Most low GI presentations in community pharmacy are self-limiting but structured assessment is still essential to identify red flags.
- Constipation is often multifactorial, with common contributors including low fibre intake, dehydration, reduced mobility and some medicines.
- Managing acute diarrhoea prioritises oral rehydration therapy, with antimotility agents used where clinically appropriate.
Constipation
Constipation is common, affecting around one in seven adults and up to one in three children.2 Prevalence increases with age, affecting 30-40% of people aged over 60 years.3 Constipation is a symptom rather than a diagnosis and usually refers to infrequent bowel movements, difficulty passing stools or a sensation of incomplete evacuation.
It is important to establish what patients mean when they describe themselves as constipated.
Reported bowel frequency varies considerably: one 1965 study of 1,055 individuals not seeking medical advice found that virtually all (99%) had bowel movement frequencies between three times a day and three times a week.4 For many patients, self-diagnosed constipation reflects a change from their usual bowel pattern.
Causes
Constipation may be primary (functional) or secondary. Primary constipation may be idiopathic or arise from a problem with the colon. Secondary constipation has an identifiable cause, such as a lifestyle change, underlying illness or medicines, as shown in Panel 1.
Other potential causes include spinal or pelvic nerve injury, intestinal disorders such as irritable bowel syndrome, and anorectal disease, such as anal fissure.
In addition, constipation is considered acute if it lasts less than three months, or chronic if it persists beyond three months.
Panel 1: Common causes of secondary constipation
- Low/inadequate fibre or fluid intake
- Immobility or lack of exercise
- Limited privacy when using a toilet
- Older age
- Female sex/pregnancy
- Anxiety or depression
- Eating disorders
- Somatic symptom disorder (where individuals have excessive thoughts/feelings over physical symptoms)
Patient assessment
Managing constipation depends on identifying the underlying cause. Pharmacy teams should take a detailed history and ask targeted questions [Table 1, below] to establish the patient’s baseline bowel pattern and identify likely contributing factors. Stool consistency is also important because it reflects GI transit time.
Table 1: Questions to ask patients with constipation
| Question | Rationale |
|---|---|
| Have there been any changes to your diet or routine? | Insufficient fibre, fluid intake or physical activity is a common cause; changes in routine may also precipitate symptoms. |
| Is there pain or blood on defaecation? | This may suggest a local anal problem, such as a fissure or haemorrhoids. |
| Is there tiredness, nausea, vomiting or loss of appetite? | These symptoms may indicate a metabolic problem, such as hypercalcaemia. |
| Is there associated weight loss or an unexplained change in bowel habit? | This may indicate colorectal cancer, particularly in patients aged over 40 years. |
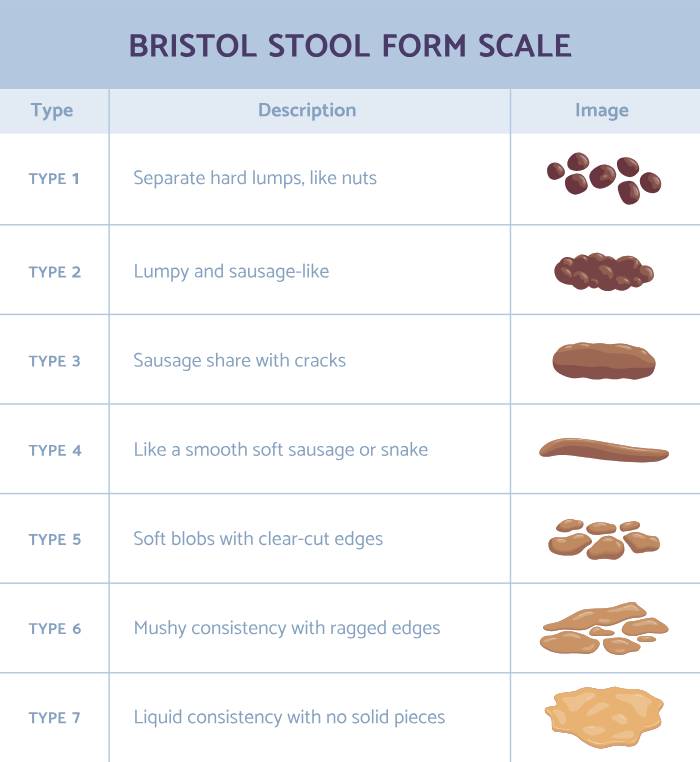
The Bristol Stool Chart, first described in 1997, rates stools from type 1 to type 7 [see below]. Type 1 describes separate hard lumps, whereas type 7 is liquid without solid pieces, indicating rapid GI transit. The ideal stool is usually type 3 or 4: sausage-shaped with surface cracks, or soft blobs with clear-cut edges.
Potential red flags
Patients with the following symptoms should be referred to their GP:
- Severe or persistent pain in the abdomen or rectum
- Blood in the stool or bloody stools
- Weight loss
- Sudden change in bowel habit, defined as any lasting deviation from the individual’s normal pattern.
NHS Bowel Screening Programme
The NHS Bowel Cancer Screening Programme started in July 2006 and has since expanded to include anyone aged 50 to 74. Screening using the faecal immunochemical test (FIT) was introduced in England in June 2019 and is designed to detect traces of blood in stools.
Results are normally available within two weeks, and although the test does not indicate the presence of bowel cancer, the presence of blood might also be caused by bowel polyps or an anal fissure. Nevertheless, those with a positive result are advised to undergo a colonoscopy.
Those with a negative test are re-screened every two years, although it is important to recognise that a negative result does not provide a high degree of certainty that bowel cancer is not present – just that it is much less likely.
According to the NHS, for every 100 people screened, 97–98 do not need further tests.
Treatment: initial self-management advice
Dietary and lifestyle changes should be suggested, such as increased consumption of high-fibre foods (including fruits, vegetables, whole wheat and bran) and adequate fluid intake.
A high-fibre diet helps normalise bowel movements by increasing stool weight and size, softening stools and supporting easier passage through the colon. Fluid intake should also be adequate. According to the British Dietetic Association, adult men should aim for at least 2,000ml of fluids daily and women 1,600ml every day.5 Pale straw-coloured urine is a useful indicator of sufficient fluid intake.
Increased physical activity can also stimulate intestinal contractions, helping stools move more easily through the lower GI tract.
Drug treatment: first-line
Bulk-forming laxatives (e.g. ispaghula husk), which increase faecal mass and stimulate peristalsis, are recommended for initial management.
These should be taken either in the morning or later in the day but avoided before bed since bowel activity decreases at night, increasing the risk of intestinal obstruction. Bulk-forming agents should be avoided in opiate-induced constipation due to the risk of faecal impaction.
Drug treatment: second-line
If stools remain hard or dry, an osmotic agent (e.g. lactulose), which retains fluid in the bowel and stimulates peristalsis, is advised, although maintenance of adequate fluid intake is still required.
Where stools become soft but remain difficult to pass, adding a stimulant laxative (e.g. senna) will help.
In addition to oral agents, faecal softeners such as docusate sodium and glycerol suppositories can be used to allow water and lipids into the stools and support easier passage. Rectal laxatives, including glycerin suppositories, may also be considered where appropriate.
Stopping laxatives
Patients should gradually reduce laxative intake once stools are soft and formed, without straining, at least three times per week. Adherence to dietary and lifestyle recommendations should be reinforced.
Constipation in children
Up to a third of children experience constipation,6 which can cause considerable parental anxiety. Children typically present with infrequent bowel evacuation, large stools, and difficult or painful defaecation. Serious underlying causes should be excluded and children with the following symptoms should be referred:
- Symptoms appearing from birth or during the first few weeks of life
- Abdominal distension with vomiting
- Ribbon-like stools, i.e. very thin or flat.
Management
Diet and lifestyle measures can help, although they should not be used in isolation. A macrogol is the recommended first-line treatment, with dosage adjusted according to response.
A stimulant laxative can be added to a macrogol, or used as an alternative if first-line treatment is ineffective. If stools remain hard, lactulose or another softening laxative, such as docusate sodium, can be added.
Treatment should be continued for several weeks after a regular bowel movement has been established and tapered gradually rather than abruptly stopped.
Diarrhoea
The World Health Organization defines diarrhoea as the passage of three or more loose or liquid stools per day, or more frequent passage than is normal for an individual, lasting less than 14 days.7
Estimates of the current prevalence of diarrhoea in the UK vary, but a 2012 study reported up to 17 million cases and 1 million GP appointments for acute infectious intestinal disease.8 Diarrhoea may be acute, lasting less than two weeks, or chronic, lasting longer than two weeks.
In community pharmacy, most patients self-diagnose acute diarrhoea, but assessment remains important to clarify the nature of symptoms and identify potential red flags.
Causes
The most common cause of acute diarrhoea is infection, with most primary care cases caused by viruses, e.g. norovirus, which is responsible for 18% of global cases of diarrhoeal disease.9 However, bacteria including Salmonella species, Campylobacter jejuni, Shigella species and Escherichia coli can also cause diarrhoea.
Acute diarrhoea can also occur because of drug therapy. Treatments typically causing diarrhoea include allopurinol, angiotensin-II receptor blockers, antibiotics, chemotherapy, magnesium-containing antacids, metformin, and selective serotonin reuptake inhibitors.
Patient assessment
Consider diarrhoea in patients who describe passing three or more loose or liquid stools over 24 hours, or more frequently than is normal for the individual. The onset of symptoms can sometimes provide clues to the underlying cause:
- Onset within six hours suggests a bacterial cause (food poisoning), while viral gastroenteritis tends to cause symptoms from 12 hours
- More frequent stools, combined with systemic symptoms (e.g. fever, vomiting), support the diagnosis of an infectious cause.
Asking about recent substance misuse, surgery, sexual practices and occupation can also help to identify a likely cause. Diarrhoea may be more likely in people working in day care centres or nursing homes.

Potential red flags
Patients with the following symptoms should be referred to their GP for further assessment:
- Any unexplained weight loss
- Rectal bleeding
- Recent hospital or antibiotic therapy
- Blood or mucus in the stools
- Nocturnal symptoms
- Recent foreign travel (other than Western Europe, North America, Australia or New Zealand).
Management: first-line
Oral rehydration to reduce the risk of dehydration is the recommended first-line approach. Adjunctive treatment with co-phenotrope (atropine 25mcg and diphenoxylate 2.5mg) can also be used.
Second-line
The antimotility agent loperamide has become
the standard therapy, particularly when rapid control of diarrhoea is needed. Bismuth subsalicylate is a suitable alternative to loperamide but has a slower onset of action.
Traveller’s diarrhoea

Cases of suspected traveller’s diarrhoea should be referred to the GP, where common first-line treatments include azithromycin, combined with oral rehydration therapy.
Diarrhoea in children
Infectious diarrhoea in children is usually viral, most commonly rotavirus or norovirus. Most children with acute diarrhoea can be managed with early and adequate oral rehydration. Infants aged under 6 months are at greatest risk of dehydration. Young patients with chronic diarrhoea (lasting more than two weeks) should be referred to their GP.
Irritable bowel syndrome
Irritable bowel syndrome (IBS) is a complex disorder of gut-brain interaction characterised by recurrent abdominal pain and altered bowel habit, including constipation, diarrhoea or both. It is common and, according to NICE, affects an estimated 5-20% of the general population,8 with a peak in people aged 20-30 years.
IBS can also be categorised based on the main stool type, so that patients can have:
- Diarrhoea-predominant IBS
- Constipation-predominant IBS
- Mixed (fluctuating between the above two types).
Causes
The absence of a single identifiable cause suggests that IBS has multifactorial pathophysiology. It is, in essence, a disorder of altered intestinal motility in which episodes may be triggered by environmental factors, such as life stress, and luminal factors, including certain foods, bacterial overgrowth or toxins, gut distension or inflammation. This altered reactivity can lead to pain, constipation, diarrhoea or a combination of these symptoms.
Patient assessment
A diagnosis of IBS is based on the presence of specific symptoms, and while pharmacy teams are not expected to make a definitive diagnosis, IBS is likely where an individual presents with a six-month history of either:
- Abdominal pain or discomfort
- Bloating
- Change in bowel habit.
Additional diagnostic clues include abdominal pain relieved by defaecation, altered stool form, such as hard, lumpy, loose or watery stools, and at least two of the following:
- Altered stool passage, such as straining, urgency or incomplete evacuation
- Abdominal bloating, distension, tension or hardness
- Symptoms aggravated by eating
- Rectal passage of mucus.
Potential red flags
Alarm symptoms include:
- Unintentional and unexplained weight loss
- Rectal bleeding
- Change in bowel habit in those over the age of 60 years
- Persistent or frequent bloating in females (especially if aged over 50 years)
- Family history of bowel cancer, ovarian cancer, coeliac disease, or inflammatory bowel disease.

Management
Patients should be informed that IBS is a chronic condition which can flare due to several factors, including stress, illness and even certain foods.
Dietary intervention: FODMAPS
Regular, balanced meals and adequate fluid intake can help. One study found that 84% of patients with IBS reported symptoms associated with at least one food source.9
A potentially beneficial dietary approach is a low fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) diet. FODMAPs are short-chain carbohydrates found in many foods, including fruit, vegetables, grains, cereals, nuts, legumes, lentils, dairy products, and manufactured foods.
A recent umbrella review concluded that a low-FODMAP diet reduces symptoms and improves quality of life in patients with IBS.10 However, the same analysis found no significant effect on abdominal pain, stool consistency, stool frequency or microbiota, which is an important limitation. In practice, patients are best referred to a dietitian for advice on FODMAP diets.
Pharmacological therapy
For patients with constipation-predominant IBS, bulk-forming laxatives, which contain soluble fibre, can be helpful. Other laxatives (except lactulose, which can cause bloating) can also be used. Conversely, those with diarrhoea-predominant IBS can take antimotility agents such as loperamide.
Other commonly used treatments
These include antispasmodic agents, e.g. mebeverine hydrochloride, alverine citrate and peppermint oil. One systematic review from 2022 concluded that mebeverine was an effective treatment option in IBS, with a good safety profile and low frequency of adverse effects.11 In addition, a 2020 systematic review found that peppermint oil was one of the most effective treatments for IBS.12 Anticholinergic agents, e.g. hyoscine or dicyclomine, are also used.
Antispasmodic agents are more useful for patients who experience pain and bloating13 (see below). There is little evidence to guide treatment choice, although drugs such as mebeverine, alverine, or peppermint oil are less likely to cause adverse effects than anticholinergics.
Probiotics
A 2025 meta-analysis of 16 randomised trials examining probiotics in IBS showed clinically significant overall improvement compared with placebo. The authors concluded that probiotics were a safe and effective supplemental treatment for patients with IBS.14 Although no specific probiotic mixture is currently recommended, NICE advises patients to try a probiotic for at least four weeks to assess effectiveness.
Bloating
Bloating refers to a subjective sensation of gassiness, trapped gas, pressure or distension without obvious visible distension. It is extremely common, with an estimated global prevalence of 18%,15 and is also a common symptom in people with IBS.
According to a recent European consensus statement, a low-FODMAP diet can help reduce bloating symptoms. Antispasmodic agents may also help when bloating is associated with IBS. However, despite widespread use of simethicone, the European group stated that there is little objective evidence that it is effective.16
Gut microbiome
As noted earlier, a healthy gut microbiome – the collection of microorganisms residing in the gut – is increasingly recognised as an important contributor to overall gut health. The composition of the gut microbiome may influence the risk of common problems such as constipation,17 IBS18 and diarrhoea.19
Although the ideal gut microbiome has not yet been defined and substantial inter-patient variation exists, diet is clearly an important contributor to the relative abundance of microbes. Further studies are needed to define the host-microbiome landscape more clearly and support tailored nutrition strategies that promote bowel health.
References
- Homson CL, Garcia AL, Edwards CA. Prevalence of gastrointestinal symptoms in the UK adult population and perceived effects of foods. Eur J Nutr. 2025 Aug 23;64(6):265. doi: 10.1007/s00394-025-03780-0.
- NHS Inform. Available online at: www.nhsinform.scot [Accessed April 2026].
- Emmanuel A, Mattace-Raso F, Neri MC, et al. Constipation in older people: a consensus statement. Int J Clin Pract. 2017 Jan;71(1). doi: 10.1111/ijcp.12920.
- Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997 Sep;32(9):920-4. doi: 10.3109/00365529709011203.
- Fluids (water and drinks) and hydration. Available online at: www.bda.uk.com/resource/fluid-water-drinks.html [Accessed April 2026].
- Constipation in children and young people: diagnosis and management. NICE, CG99, 2017. Available online at: www.nice.org.uk/guidance/CG99 [Accessed April 2026].
- Diarrhoeal disease. World Health Organization. 2017. Available online at: www.who.int [Accessed April 2026].
- NICE (2017). Irritable bowel syndrome in adults: diagnosis and management. Available online at: www.nice.org.uk [Accessed April 2026].
- Böhn L, Störsrud S, Törnblom H, et al. Self-reported food-related gastrointestinal symptoms in IBS. Am J Gastroenterol. 2013.
- Bogdanowska-Charkiewicz D, Malinowska U, Daniluk J. Low-FODMAP diet in IBS. Front Nutr. 2026.
- Daniluk J et al. Mebeverine in IBS. 2022.
- Black C et al. IBS meta-analysis. 2019.
- BMJ Best Practice. BMJ
- Almalki AS et al. Probiotics in IBS. 2025.
- Ballou S et al. Bloating. 2023.
- Melchior C et al. Bloating consensus. 2025.
- Feng C et al. Microbiota constipation. 2024.
- Cheng X et al. Microbiota IBS. 2024.
- Ian R et al. Microbiota diarrhoea. 2025.