
In Learning
Follow this topic
Bookmark
Record learning outcomes
|
Learning objectives
After reading this feature you should be able to:
● Identify common causes of fever in children and recognise when further assessment is needed
● Apply differential diagnosis principles to help rule out serious underlying causes of fever ● Recognise red flag symptoms and provide appropriate self-care, OTC treatment and safety-netting advice |
Fever management in children is one of the most frequent queries encountered in community pharmacy. Estimates suggest that up to 40% of young children experience an episode of fever every year.1 Pharmacy teams therefore have an important role in reassuring concerned parents, recommending appropriate treatments and providing clear safety-netting advice.
Fever: first steps
When a parent presents with a feverish child, the first step is to confirm whether the child has a fever. Fever is defined as a temperature of 38°C or higher. Children with fever may feel hot to the touch, particularly on the forehead, back or chest. They may also appear flushed, sweat more than usual, shiver, have a reduced appetite or seem generally unwell.
Accurately measuring body temperature in very young children can be difficult. For babies aged under four weeks, NICE advises using an electronic thermometer placed in the armpit. For older children, a digital thermometer placed in the ear is usually the easiest and most accurate approach.
It is important to remember that if parents have already given an antipyretic, such as ibuprofen or paracetamol, body temperature may have returned to normal. However, the underlying illness that caused the fever may still be present.
|
KEY FACTS
● Fever is common in children and is usually caused by a viral infection
● Differential diagnosis should include common viral illnesses, bacterial infections such as a UTI, otitis media and tonsillitis, and rare but serious conditions such as bacterial meningitis ● Parents should seek medical advice for a temperature of 38°C or higher in babies under 3 months, 39°C or higher in infants aged 3–6 months, or any fever lasting more than 5 days ● OTC antipyretics such as paracetamol and ibuprofen can reduce fever and associated pain when used at age-appropriate doses |
Fever is one of the body’s characteristic responses to infection, so its potential underlying causes are numerous. The main triggers in children are viral infections such as colds, flu and norovirus, as well as childhood illnesses such as chickenpox, respiratory syncytial virus (RSV), and hand, foot and mouth disease.
Less commonly, fever may be due to a bacterial infection such as tonsillitis or a urinary tract infection.
To help identify the underlying cause of a child’s fever, pharmacists should ask about associated signs and symptoms. These may include pain, cough, nausea or vomiting, breathlessness, itching, rash, swelling, or signs of confusion.
Pain associated with fever is often a key indicator that can point towards the correct diagnosis. For example, sore throat and earache are most likely to be caused by a cold or other simple viral infection, although severe cases may indicate tonsillitis or bacterial otitis media. Stomach pain accompanied by gastrointestinal symptoms may point to a viral infection such as norovirus.
With any feverish child, it is also important to establish if they have any underlying health conditions or are receiving any current medical treatments. Children being treated with immunosuppressant medication or with a known immunodeficiency may be more susceptible to infections and more at risk of complications from a febrile illness.
Pharmacists should also be aware of potential non-infectious causes of fever. For example, young infants may develop a slightly raised body temperature when teething. Childhood vaccinations can also cause mild fever in the 24 to 48 hours after administration as the immune system mounts its primary response.
In some cases, young babies may simply be over-wrapped or overdressed, particularly as the weather becomes warmer, which can raise core body temperature.
Differential diagnosis
Undoubtedly the most important part of the fever differential diagnosis is to rule out other less common – but more serious – illnesses that can cause fever in children. Fever is second only to breathing difficulties as the most common cause of hospital admission among children.1
Meningitis

Meningitis is a general term describing inflammation of the protective membranes around the brain and spinal cord, usually triggered by a bacterial or viral infection.2 Viral meningitis is the most common type and is usually mild, resolving without treatment within 7-10 days.
The most common causative viruses are enteroviruses, which tend to peak in the summer and early autumn months.2
In contrast, bacterial meningitis and meningococcal disease are rare but potentially life-threatening causes of fever in babies, children and adolescents. Serious complications can include hearing impairment, limb loss or sepsis.
Bacterial meningitis can result from infection with several types of bacteria, while meningococcal disease is specifically caused by Neisseria meningitidis, the most common cause of bacterial meningitis in the UK. Six main strains, or serogroups, can cause meningitis: A, B, C, W, Y and X.
Of these, strain B is the most common cause of meningitis and invasive meningococcal disease, where infection progresses to overt sepsis.2
Parents of teenagers may be particularly concerned about meningitis B following recent high-profile outbreaks at UK universities that led to several deaths.3 Bacterial meningitis can worsen rapidly, so early recognition of signs and symptoms is important. However, meningitis B symptoms can mimic other common illnesses, such as hangover, flu or gastrointestinal upset, and may present in any order.2
Red flag symptoms of bacterial meningitis include fever, particularly with sudden onset, severe and worsening headache, neck stiffness, cold hands and feet, dislike of bright lights and altered mental state. Meningococcal disease also typically produces a non-blanching rash that does not fade when pressure is applied with a glass.
In children under 2 years of age, a bulging fontanelle may be apparent.
Any suspected case of bacterial meningitis or meningococcal disease is a medical emergency and requires immediate action. Parents should be urged to dial 999 or take their child straight to their nearest A&E department.
In June the Government announced a new community pharmacy vaccination service to provide one-off meningococcal B jabs to protect young people heading to universities or residential further education settings ahead of the start of term in autumn 2026. The start of the service is planned towards the end of this month (July).
Herpes simplex
Oral herpes simplex virus (HSV) is most associated with cold sores, which are mild and self-limiting. However, herpes infection in young babies can be very serious. Neonatal herpes may be contracted during pregnancy and delivery, or passed to the baby through contact, such as a kiss, from someone with an active cold sore.
The risk is highest in the first six weeks after birth. Sometimes the initial herpes infection causes only local symptoms, but in serious cases it can spread to internal organs, including the brain.
Pharmacists should consider possible herpes simplex encephalitis in children with fever and focal neurological signs, seizures or decreased levels of consciousness.1 Focal neurological deficits can be difficult to identify in babies, but may include muscle stiffness or floppiness, abnormal eye deviation, or asymmetry in facial movement.
Pneumonia
Although not automatically associated with children, pneumonia is a common childhood illness, with an estimated 120 million cases occurring worldwide in children under 5.4
In the UK, roughly 1 in every 300 children under the age of 5 years will get pneumonia, although this risk drops off with age.5 Children under 2 years are most susceptible due to their undeveloped immune systems. Also at risk are children with pre-existing respiratory conditions and those who did not receive the pneumococcal vaccine (which is part of the routine NHS childhood vaccination schedule).
Alongside a fever, key symptoms of pneumonia to look out for include rapid breathing, nasal flaring, and chest indrawing (retraction).
UTIs
Urinary tract infections should form part of the differential diagnosis in any baby or child under 5 years of age with fever – particularly girls, who are at higher risk. UTIs are most common among young infants and toddlers, where toilet training can increase risk factors for bladder infection, such as holding urine for long periods or incomplete voiding.
Associated signs or symptoms that increase the likelihood of a UTI include painful or more frequent urination, new bedwetting, urine that looks dark, cloudy or bloody, urine with a strong smell, and pain in the stomach or groin area.
Other causes
Septic arthritis or osteomyelitis is another potential cause of fever in children if there are signs of limb or joint swelling or pain – for example, if the child is unable to use their arm/leg or is non-weight bearing.
For a fever that has lasted longer than five days, Kawasaki disease – a rare condition associated with inflammation of the blood vessels – should be considered. This illness is most common in children under the age of 5 years and produces a persistent fever as well as other symptoms such as swollen neck glands, reddening of the palms of the hands or soles of the feet, red eyes, redness inside the mouth or on the tongue, dry and cracked lips, and a rash.
Risk assessment and safety netting
Risk assessment is one of the most challenging undertakings when faced with an anxious parent of a feverish child, yet equally the most important.
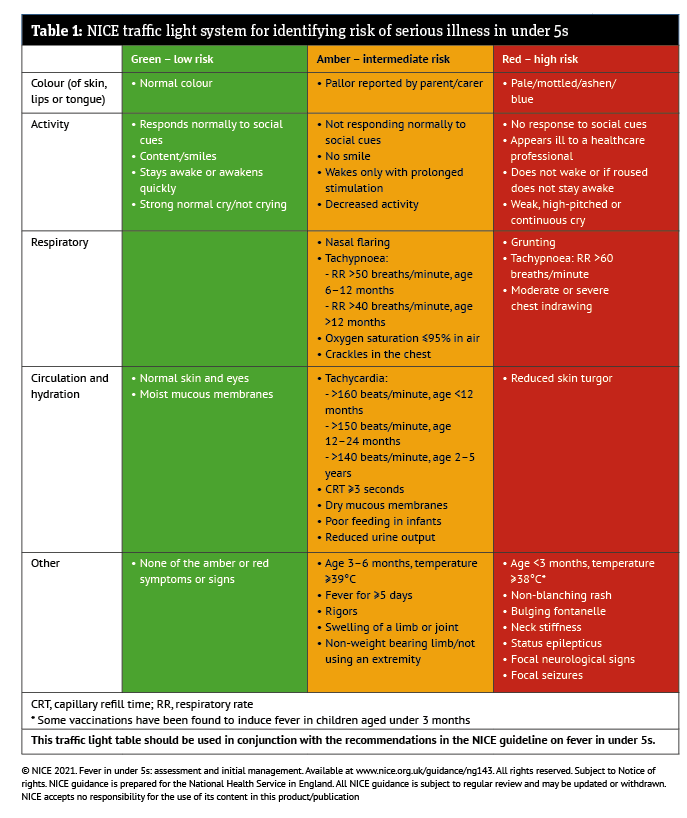
The traffic light system developed by NICE provides a useful tool for assessing the risk of serious illness in children. For infants or children in the green (low risk) category, pharmacists can reassure parents that the fever is unlikely to be due to a serious underlying cause. Key indicators that a child falls into the low-risk green zone include:
- Normal colour of skin, lips or tongue
- Normal activity levels: responds to social cues, content or smiling, awake (or awakens when roused), strong normal cry or not crying
- No unusual respiratory symptoms such as rapid breathing, grunting or chest indrawing
- Normal skin and eyes, and moist mucous membranes.
It is important to note that, in very young children, fever alone can be sufficient to place them in the higher-risk amber or red categories. A temperature of 39°C or higher, or fever lasting for 5 days or more, in an infant aged 3-6 months, is an amber risk feature and requires immediate onward referral to a GP.
In babies aged under 3 months, a temperature of 38°C or higher is a red risk feature. Parents should be advised to consult a doctor urgently within 2 hours or go straight to A&E if there are other red features suggesting a serious or life-threatening cause of febrile illness, such as sepsis or meningitis.
The NHS lists the following red flag symptoms in children as requiring parents to dial 999 immediately:
- Stiff neck
- Non-blanching rash
- Light sensitivity
- Cold hands or feet
- Changes to skin colour, such as blue, grey or blotchy skin
- Drowsiness or difficulty waking
- Extreme agitation or confusion
- Difficulty breathing, breathlessness or very fast breathing
- Not responding as normal or being disinterested in feeding or normal activities.
Above all, parents should be encouraged to trust their gut instinct when their child is unwell and has a temperature. A recent study in The Lancet Child & Adolescent Health adds to evidence that parental intuition can be a highly reliable clinical indicator, based on parents’ unique knowledge of their child’s baseline and usual behaviour.7
In this study, children whose parents expressed concern that they were getting worse were significantly more likely to experience serious illness, even when outward vital signs were normal.7
Management
Feverish children in the green zone for risk, with no amber or red features, can generally be managed at home with self-care and OTC medications.
Parents should be encouraged to offer their child regular fluids and, if still breastfeeding, continue as normal. In contrast to popular wisdom, a feverish child should not be undressed or sponged down to cool them. However, it is important to check on a feverish child regularly, including during the night, and keep them home from nursery or school until their fever has resolved.
As the mainstay of fever treatment, pharmacy teams can recommend antipyretics to help reduce body temperature and relieve associated pain or discomfort. It is important to ensure that all OTC fever-relieving products are used according to the pack instructions and that dosing is age appropriate.
Paracetamol should not be given to babies under 2 months, while ibuprofen is not suitable for infants under 3 months or weighing less than 5kg. Ibuprofen should also not be recommended if a child has chickenpox, is showing signs of dehydration or has a pre-existing diagnosis of asthma.
For younger children or those unable to swallow tablets, liquid formulations of paracetamol and ibuprofen can be recommended, while solid dose forms may be appropriate for children aged 12 years and older. Parents should be advised to use either paracetamol or ibuprofen, and not to alternate between the two unless specifically recommended by a healthcare professional.
Aspirin should never be given to children under 16 years of age because of the small but significant risk of Reye’s syndrome, which can trigger brain swelling and liver damage in children with an underlying viral infection.
Febrile seizures are a potential complication of fever in young children and result directly from elevated body temperature. They are most common between 6 months and 6 years of age, and typically last between 2-3 minutes.
The NHS advises parents to dial 999 or go to A&E if their child has a febrile seizure for the first time, if it lasts more than 5 minutes or if it recurs within 24 hours. The same advice applies if the child is having difficulty breathing, if only one side of the body is affected by the seizure, or if the child is sleepier than usual in the one-hour postictal period (the recovery phase immediately following a seizure).6
Fever can also cause dehydration by accelerating fluid loss from the body – for example, through increased sweating and higher metabolic demand. Parents should be advised to stay vigilant for signs of dehydration, including reduced urine output, such as dry nappies in babies, dry mouth, lack of tears, sunken eyes and a generally unwell appearance. If these signs develop, further medical advice should be sought.
In most cases, childhood fever resolves on its own within 1-4 days. However, parents should consult their GP if the high temperature lasts for longer than 5 days, if they are concerned that their child is becoming increasingly unwell, or if they are unable to look after them at home.
|
References
|