First person: Why were we down £50,000?
Pharmacy Magazine,
04 Feb 2021![]() 3 Min
3 Min
This site is intended for Healthcare Professionals only
Pharmacy Magazine,
04 Feb 2021![]() 3 Min
3 Min
Pharmacy Magazine,
04 Feb 2021![]() 3 Min
3 Min

We knew that we had paid over Drug Tariff prices for many items in order to obtain stock at the start of the pandemic but felt that could not equate to the £50,000 drop in gross profit — so we looked around for what else had changed. And one big change has been the prescribing via FP10MDA instalment prescriptions.
Since March the number of patient contacts has been reduced considerably by most prescribers – understandable because of their desire to avoid face-to-face contact and to address the problems some pharmacies were having in undertaking supervised consumption of Controlled Drugs at the start of the pandemic. This brought an immediate decrease in the payment for our locally commissioned support service that includes supervised ingestion of methadone. However, we realised this early and our commissioners quickly put in place a top-up payment based on pre-Covid average payments. So that was not the cause.
I decided to read the Drug Tariff carefully to check exactly how we are paid for instalment prescriptions and then look at my FP34B (our payment details) to try to decipher whether we had received those payments. I soon discovered that this is not checkable via the FP34B, but I did realise that I was getting warm.
The table below shows the Drug Tariff payments relating to methadone.
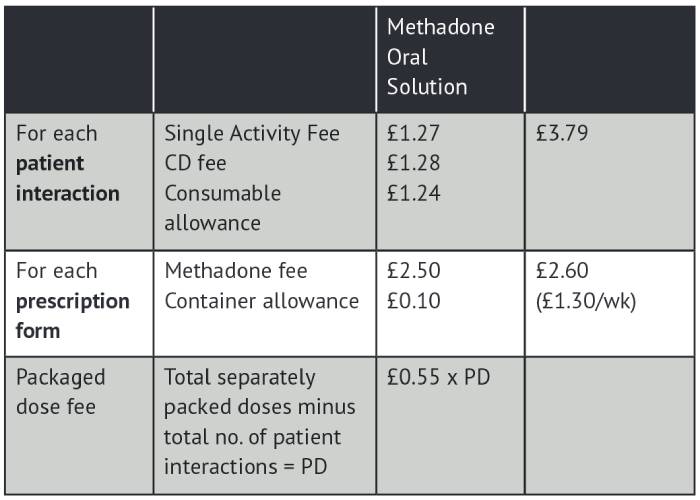
The Single Activity Fee (SAF), the Controlled Drug (CD) fee and the Consumable Allowance (CA) relating to methadone scripts add up to £3.79 per patient contact.
As a response to the pandemic the number of patient contacts relating to methadone reduced considerably. Moving from, say, 10 contacts per 14-day script to just two creates a reduction in pay of 8 x £3.79 = £30.32 per 14 days, but you gain eight Packaged Dose Fees (8 x 55p = £4.40), producing a net reduction of £25.92 per 14 days = £674 per annum per patient.
Not everyone will have seen such a drastic reduction, but I’d guess it would average out at around half of the patients. So for us, supporting 200+ methadone patients and 60 buprenorphine patients, that would be a reduction in pay for methadone patients alone of 100 x £674 = £67,400p.a. plus a reduction in pay for non-methadone instalment scripts.
The problem is that the workload remains essentially the same – or probably more in our case because we’ve gained extra patients due to the Covid-19 problems experienced at other pharmacies.
Looking at our prescription submissions of FP10MDA (Apr-Sep 2020), the number of items (patient interactions) fell 24 per cent from 18,753 last year to 14,334 this year. Our Controlled Drug fees for that period went from £20,093 to £17,836 (11 per cent down despite a massive rise in end-of-life treatment) – CD fees for methadone is per interaction, but they are not shown separately on our payment schedule.
The ‘methadone fee’, however, which is paid per prescription form and is shown on the FP34B, increased from £12,929 to £17,601 (+36 per cent). So we had new prescriptions (and patients) creating lots more work, but, because there was less direct patient contact, it resulted in a massive decrease in pay.
Add to this a possible reduction in locally paid supervised payments in some areas and you can see what a disastrous financial hit this is for pharmacies treating a high number of people for addiction. We are left with a loss-making service, which is unsustainable.
What can be done about it? My suggestion is for affected contractors to urge PSNC to request an immediate payment to compensate for the lost SAF, CD, CA fees so far. Looking forward, a simpler system that amalgamates all the fees relating to addiction treatment into one single ‘instalment prescription payment’ paid per form would make it fairer and far clearer for pharmacy contractors to monitor.
I doubt if many contractors have fully realised the implications of the reduction in supervised doses as it is impossible to extract the information from the FP34B payment schedule. Many have been negotiating with local commissioners trying to protect their ‘supervision fees’ without realising that a much bigger problem relates to Drug Tariff payments. Once contractors do realise this, they will seriously consider pulling out of the service because it has become another loss-making activity on top of all the other pandemic costs that have yet to be reimbursed.
Funding relating to the dispensing of instalment prescriptions involves two payments.
The national payment via the NHS Drug Tariff covers the remuneration for the cost of the medication along with various payments to cover the cost of basic dispensing, staff, premises and all the other costs involved in running a pharmacy. This is part of the Community Pharmacy Contractual Framework (CPCF) and involves negotiations between PSNC on one side and the DHSC and NHSE on the other.
Instalment prescriptions took a big hit back in 2012 when an attempt was made to “simplify” the Drug Tariff, which as you might guess, made it even more complicated! Changes were made to the payment structure for methadone dispensing. We were assured it was “cost neutral”, but either by accident, or design, it certainly wasn’t and funding moved out of addiction payments and into other services.
The second payment is a local payment and covers other aspects relating to instalment prescriptions above and beyond simple dispensing (e.g. supervised doses, feeding back missed doses, liaising with the prescribing team, health promotion). In our case this payment is negotiated between Sheffield DACT and Sheffield LPC.
More take-home doses results in less supervision and the payment is related to the number of supervisions. This produced a big drop in income for some pharmacies, which Sheffield DACT were quick to recognise and they have lessened this considerably by the introduction of a top-up payment based on previous averages until a more holistic service specification is in place – hopefully by April 2021.