
In Learning
Follow this topic
Bookmark
Record learning outcomes
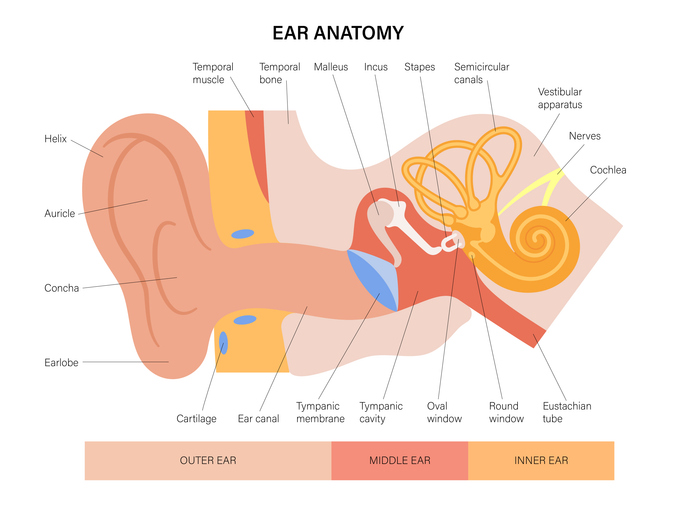
Before focusing on specific ear problems, it is helpful to understand basic ear anatomy and function. The ear comprises three parts: the outer (external) ear, a middle air-filled cavity and the inner fluid-filled ear.
The external ear is primarily composed of bone and cartilage. The outer two-thirds of the ear canal contains tiny hairs, while the inner third, leading to the eardrum, is lined with smooth skin containing glands that secrete cerumen (earwax). At the end of the external auditory canal lies the tympanic membrane (eardrum), a thin structure that moves in response to pressure changes.
Behind the tympanic membrane sits the middle ear, connected to the nose via the Eustachian tube. It contains three tiny bones that transmit sound vibrations.
The inner ear contains the cochlea, the organ of hearing. The cochlear nerve houses thousands of hair cells that convert mechanical vibrations into electrical signals interpreted by the brain. The inner ear also includes the vestibule and semicircular canals, which detect movement and help maintain balance.
Each part of the ear can be affected by different conditions and pharmacy teams should be familiar with presenting symptoms to help identify the likely origin.
After reading this learning update on common ear problems, you should be able to:
- Recognise ear conditions affecting the outer, middle and inner ear, and differentiate between them based on symptoms
- Advise on appropriate treatments and self-care
- Identify red flags and know when referral to a GP or access to a Pharmacy First service is appropriate
External ear
Otitis externa
The external ear consists of the pinna and the external auditory meatus (ear canal). Otitis externa (OE) is a common condition, usually caused by bacterial infection. It presents as diffuse inflammation of the ear canal and may also involve the pinna or tympanic membrane.
Key symptoms: Itch, pain on tragus movement, canal inflammation, fullness, with or without hearing loss, swelling and/or discharge.
A common predisposing factor is prolonged exposure to water, hence the term ‘swimmer’s ear’, as trapped water creates an environment for bacterial growth.
Differential diagnosis: Atopic and seborrhoeic eczema affecting the ear canal can mimic OE, typically presenting with erythema, xerosis and lichenification. However, OE is usually more painful.
Otitis media should also be considered. Examination with an otoscope helps differentiate conditions. Pain on movement of the pinna or pressure on the tragus is typical of OE but not otitis media.
Management: Self-care advice includes keeping the ear clean and dry, and avoiding swimming for 7-10 days if necessary. OTC treatments include:
- Acetic acid 2%, which acts as an astringent by lowering pH and inhibiting microbial growth
- Aluminium acetate, which similarly acidifies the ear canal.
Both have comparable efficacy to topical antibacterial/steroid combinations over seven days, although effectiveness may reduce with prolonged use.
- Pharmacy teams see a range of common ear problems affecting the outer, middle and inner ear
- External ear problems can often be treated with OTC products
- Middle ear problems, such as otitis media, are treatable via Pharmacy First and similar schemes
- Inner ear conditions, including vertigo and tinnitus, require GP referral
Referral: Refer to a GP if:
- There is generalised inflammation of the pinna (possible perichondritis)
- Hearing is impaired, particularly in children (possible glue ear)
- There is mucopurulent discharge or systemic upset (possible otitis media)
- Any growth is present on the pinna, especially in older adults.
Earwax
Cerumen is a hydrophobic substance produced in the ear canal. It protects by trapping debris, lubricating the skin and providing antimicrobial activity.
It is composed of lipids, desquamated skin cells (around 60%), proteins and antimicrobial peptides. Normally, it is cleared naturally through jaw movement. However, accumulation can occur due to cotton bud use, digital manipulation or hearing aids, which may push wax deeper into the canal.
Untreated build-up can lead to hearing loss and discomfort, though complications are rare.
Key symptoms: Fullness, hearing loss, sometimes tinnitus
Management: OTC softening agents include:
- Olive or almond oil
- Sodium bicarbonate
- Proprietary preparations.
These should be used several times a day for up to five days. Evidence does not support one product over another – indeed, a 2018 Cochrane review found no clear product superiority.
Middle ear
Acute otitis media
Acute otitis media (AOM) is a very common infection, particularly in children. By three years of age, 50-85% of children will have experienced at least one episode. Older children typically present with earache, while younger children may show ear tugging or rubbing. Non-specific symptoms include fever, irritability, poor feeding and respiratory symptoms.
Key symptoms: earache, fever, ear tugging, red or bulging tympanic membrane, possible perforation and discharge.
Management: Around 60% of cases resolve spontaneously, usually within three days.
Pain relief with paracetamol or ibuprofen is recommended. Under Pharmacy First in England, pharmacists can perform otoscopic examination. Typical findings include a red, cloudy or bulging tympanic membrane and loss of normal landmarks.
Amoxicillin is first-line antibiotic therapy where needed, though delayed prescribing may be appropriate in selected patients.
(See panel below on ‘Diagnosis and management of acute otitis media in children’)
- Earache is a common event in children and is usually associated with a cold or flu-like viral illness. When there are signs of eardrum inflammation, this is called acute otitis media (AOM). Most children will have at least one episode of AOM in the first few years of their life
- Younger children may hold or rub their ear, or may have non-specific symptoms such as fever, crying, poor feeding, restlessness, cough or rhinorrhoea
- In many children and young people symptoms resolve rapidly and over 80% of AOM cases settle without antibiotic treatment in about three days
- Common complications of acute otitis media include recurrence of infection, hearing loss (which is usually temporary) and perforated eardrum. However, antibiotics make little difference to the incidence rates of these problems
- Most cases can be managed with pain relief medication – paracetamol or ibuprofen plus self-care
- In patients with moderate and severe symptoms without eardrum perforation, consider offering phenazone 40mg/g with lidocaine 10mg/g ear drops for up to seven days (subject to inclusion/exclusion criteria in PGD) plus self-care
- Antibiotics provide greater benefit in children under two years if both ears are affected (bilateral AOM) or where there has been a perforation of the eardrum and discharge of pus (otorrhoea). Pharmacy First and similar schemes in the UK enable the supply of antibiotics in these cases
- To provide a service for managing AOM, pharmacists need to gain experience and competence in using an otoscope
Eustachian tube dysfunction
The Eustachian tubes regulate pressure across the eardrum. Dysfunction occurs when they fail to equalise pressure, often due to upper respiratory tract infection.
Key symptoms: Inability to ‘pop’ ears, muffled hearing, discomfort during pressure changes (e.g. flying).
Management: Symptoms are usually mild and self-limiting. Advice includes swallowing, yawning or chewing to equalise pressure. Nasal decongestants or oral antihistamines may provide relief.
Inner ear
Tinnitus
Tinnitus is the perception of sound without an external source. It affects around one-third of people at some point, with a global prevalence of 10-15%. While not life-threatening, it can significantly impact quality of life.
Key symptoms: Ringing, buzzing, hissing, clicking, pulsing or humming sounds.
Management: There are no approved pharmacological treatments for tinnitus. Pharmacists should examine the ear to exclude causes such as earwax or otitis media with effusion. If no cause is identified, refer to a GP. Many cases improve over time or with treatment of an underlying condition.
Vertigo
Vertigo is a symptom characterised by a sensation of movement or spinning. It differs from general dizziness, which describes light-headedness without a sense of motion. Prevalence is estimated at 3-10%.
Key symptoms: Sensation of spinning or movement; loss of balance; unsteadiness or difficulty walking.
Management: Patients presenting with vertigo should be referred to a GP for full assessment. Important differentials include:
- Presyncope (feeling faint)
- Disequilibrium (imbalance or unsteadiness).

A 36-year-old patient, Elaine, complains of pressure, fullness and muffled hearing in the right ear for two days and requests earwax removal.
The patient reports a “low humming” noise and intermittent episodes of dizziness, during which the room feels like it is spinning, lasting 30 minutes to two hours.
The patient’s partner notes that the television volume has increased, although sounds are still perceived as muffled. What do you advise?
Answer
The patient should be referred to a GP, as the triad of vertigo, hearing loss and tinnitus is suggestive of Ménière’s disease (MD). Vertigo episodes are typically sudden, incapacitating, and last from minutes to hours.
There is no cure for MD, but lifestyle measures may help. These include reducing salt intake to limit fluid retention within the inner ear. Some patients report symptom worsening after salty meals. The NHS also advises reducing caffeine and foods such as chocolate, although high-quality evidence is limited.
Medicines such as antihistamines (e.g. cinnarizine, cyclizine, promethazine) or phenothiazines (e.g. prochlorperazine) may help during acute attacks. Prophylactic betahistine is often used to reduce the frequency and severity of symptoms.
Patients like Elaine should be advised not to drive during symptomatic periods. Prognosis often worsens over time, with vertigo episodes decreasing but hearing loss and tinnitus progressing. It has been estimated that bilateral, severe hearing loss occurs in 1–6% of patients. In addition, there is an increased risk of falls among those who experience imbalance and unsteadiness.