In Clinical
Follow this topic
Bookmark
Record learning outcomes
Key counselling points
- Identify: Mechanical vs inflammatory pain; watch for red flags
- Advise: Exercise, posture, weight management, use topical NSAIDs first-line
- Refer: Promptly if severe, persistent or inflammatory symptoms
Learning objectives
After reading this feature, you will be able to:
- Distinguish between mechanical and inflammatory joint pain
- Recognise the key features of osteoarthritis, rheumatoid arthritis and gout
- Provide evidence-based advice on both pharmacological and non-pharmacological management of muscle and joint pain
- Identify red flags and know when referral is required.
With musculoskeletal (MSK) problems accounting for substantial morbidity and lost productivity in the UK, community pharmacists’ role in early recognition and effective management is increasingly important. This article provides an overview of the most common joint and muscle-related conditions encountered in pharmacy, how they present, and how pharmacists can support patients safely and effectively.
What is joint pain?
Joint pain, or arthralgia, is a broad term used to describe discomfort such as aching or soreness within a joint. It forms a major component of musculoskeletal health, which also encompasses bones, muscles, ligaments and connective tissues.
Musculoskeletal conditions are extremely common, with data suggesting that in 2024, 18 per cent of those aged 16 years and over self-reported a long-term MSK condition. The wider impact is substantial, with more than 30 million working days estimated to be lost each year as a result of MSK problems.
The two principal causes of arthralgia are mechanical and inflammatory, and distinguishing between these is central to effective pharmacy assessment.
Mechanical joint pain arises as a result of wear and tear. Joints are exposed to continual low-level damage through everyday activity and rely on ongoing repair mechanisms. Mechanical joint pain is therefore the most common form of this type of pain. It is typically worsened by movement and relieved by rest.
The most frequent cause is osteoarthritis.
Although the precise cause remains unclear, osteoarthritis (OA) is characterised by the gradual breakdown of the protective cartilage surrounding a joint and a failure to regenerate it. As cartilage is lost, bone-on-bone friction occurs during movement, leading to pain and stiffness.
Increasing age is a major risk factor, with the condition far more prevalent in people over 45 years of age. Genetics, obesity, previous joint injury, occupational stressors and female sex also increase risk.
Osteoarthritis most commonly affects the knees, hips and hands. Patients often describe tenderness and swelling around the joint, sometimes accompanied by a grating or cracking sensation on movement. As the condition progresses, everyday activities such as climbing stairs, gripping objects or getting dressed can become increasingly difficult.
Symptoms typically develop slowly over months or years and often begin with pain related to activity.
Diagnosis and management of osteoarthritis
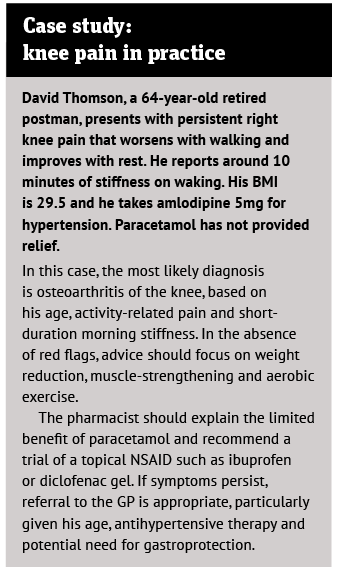
According to NICE guidance, osteoarthritis can be diagnosed clinically without the need for imaging in patients aged 45 years or over who have activity-related joint pain and either no morning stiffness or stiffness lasting no longer than 30 minutes. This allows pharmacists to confidently recognise likely OA presentations and offer appropriate initial advice.
The primary aim of treatment is to reduce pain and stiffness while improving joint function. Non-pharmacological measures form the foundation of management and should be recommended to all patients. Therapeutic exercise and, where appropriate, weight management can significantly reduce joint load, particularly in weight-bearing joints such as the knees.
Combining exercise with dietary changes has been shown to reduce pain while increasing muscle mass.
Patients frequently ask about glucosamine and chondroitin sulphate. Although these supplements are not recommended by NICE, a recent meta-analysis involving nearly 4,000 patients found that the combination was effective for knee osteoarthritis compared with placebo, albeit with many low-quality trials included. A trial of supplementation may therefore be reasonable, with continuation if benefit is observed.
From a pharmacological perspective, topical non-steroidal anti-inflammatory drugs are effective and recommended as first-line treatment. Patients should be advised that their full benefit may take up to two weeks to take effect.
Capsaicin cream is an alternative option. If topical treatments provide insufficient relief, oral NSAIDs may be considered where there are no contraindications – although referral to the GP may be more appropriate in older patients or those with comorbidities.
The evidence supporting paracetamol or weak opioids such as codeine is less robust, and these should not be routinely used except for short-term relief. More potent opioids have not been shown to provide clinically meaningful benefit in hip or knee osteoarthritis.
Some specialists suggest using natural alternatives to traditional painkillers to help manage joint discomfort and reduce side-effect risk – for instance, compounds with anti-inflammatory properties derived from rose-hip, presented in supplement form.
Recognising red flags
While most presentations of osteoarthritis can be managed in pharmacy, pharmacists should remain alert to red flags, including signs of infection, prolonged or severe morning stiffness, inability to move a joint or bear weight, and neurological symptoms such as tingling or numbness. These warrant prompt referral.
Inflammatory joint pain
Inflammatory joint pain arises from immune or metabolic causes and results in inflammation of the joint lining. Unlike mechanical pain, it is characterised by swelling, warmth and significant morning stiffness. Although less common, affecting around 1 per cent of UK adults, prevalence increases with age.
The most common inflammatory joint conditions seen in practice are rheumatoid arthritis and gout.
Rheumatoid arthritis is an autoimmune disease involving chronic inflammation of the synovium, leading to progressive joint and periarticular damage. It affects around 1 per cent of the UK population and is between two and four times more common in women.
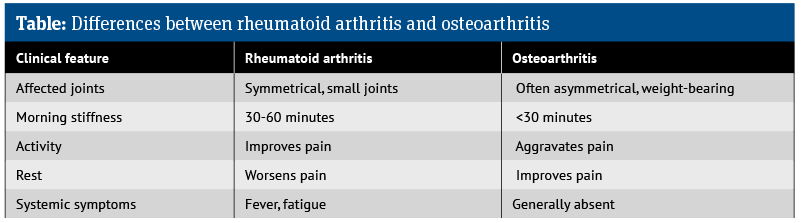
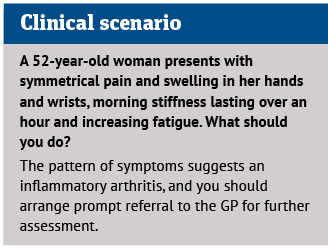
Rheumatoid arthritis typically presents with symmetrical involvement of the small joints of the hands, wrists and feet, accompanied by morning stiffness lasting between 30 and 60 minutes. Pain often improves with activity and worsens with rest, and systemic features such as fatigue may be present.
Prompt referral for assessment and initiation of disease-modifying anti-rheumatic drugs, such as methotrexate, leflunomide or sulfasalazine, is essential.
Gout results from hyperuricaemia and deposition of monosodium urate crystals in and around joints, leading to sudden, severe flares of pain, heat and swelling. It is more common in men and typically affects distal joints, most commonly the big toe.
Pharmacists can play a key role in early recognition. Patients may describe sudden onset of excruciating pain, often developing overnight, with a hot, red, swollen joint that is exquisitely tender to touch. Any presentation suggestive of gout should be referred.
Acute attacks are treated with oral NSAIDs or colchicine, while long-term management involves urate-lowering therapy such as allopurinol or febuxostat. Lifestyle advice, including reducing alcohol intake, limiting purine-rich foods and encouraging weight loss, is commonly recommended, although high-quality supporting evidence is limited.
Muscle pain
Muscle complaints commonly seen in pharmacy fall into two broad categories: acute injuries such as sprains and strains, and lifestyle-related tension, often referred to as office syndrome.
Sprains involve ligament injury around joints, most commonly the ankle, knee, wrist or thumb, while strains involve muscle or tendon injury, frequently affecting the thigh, back or foot. Most mild injuries resolve within a few weeks.
Initial pharmacy management includes paracetamol or topical NSAIDs, alongside advice on PRICE self-management during the first 24 to 72 hours.
Poor workstation design is a frequent cause of neck, upper back and lower back pain. Pharmacists can offer practical advice on posture, screen height, seating position and the importance of regular movement. Standing or moving every 30 minutes helps lubricate joints and restore blood flow to muscles.
In addition to topical NSAIDs, local heat or cold application has good evidence for improving pain and physical function. Any patient reporting numbness, pins and needles or weakness should be referred to exclude nerve compression.
Non-pharmacological approaches
Lifestyle choices play a central role in relieving joint and muscle pain and helping people stay active. Research suggests that one of the most effective strategies is regular, gentle exercise supported by physiotherapy such as walking, swimming and yoga.
According to consultant rheumatologist Dr Rod Hughes, activities like these keep joints moving and help strengthen the muscles and ligaments that support them, which in turn reduces stiffness and takes pressure off painful joints. “It’s also important to balance activity with rest. Alternating heavier tasks with periods of recovery helps prevent flare-ups caused by repetitive stress and overuse,” he says.
Maintaining a healthy body weight is also especially important for managing pain. Extra weight increases the load on joints, particularly in the knees and hips, which worsens pain and speeds up joint wear. “Even small reductions in weight can significantly reduce pain and improve movement,” says Hughes.
“Diet can also influence inflammation and pain levels. Eating plenty of fresh fruit and vegetables, whole grains, nuts and seeds, along with at least two portions of oily fish per week, provides antioxidants and omega-3 fats that can help reduce inflammation and protect against cell damage,” he adds.
Summary
Joint and muscle pain are core elements of everyday pharmacy consultations. By distinguishing between mechanical and inflammatory causes, offering evidence-based self-care and treatment advice, and recognising red flags, pharmacists can make a meaningful difference to patient outcomes while supporting appropriate use of primary care services.