In Clinical
Follow this topic
Bookmark
Record learning outcomes
Headaches are a common complaint among the general population. In fact, according to NICE, more than 10 million people in the UK experience regular or frequent headaches, accounting for around one in 25 GP consultations.
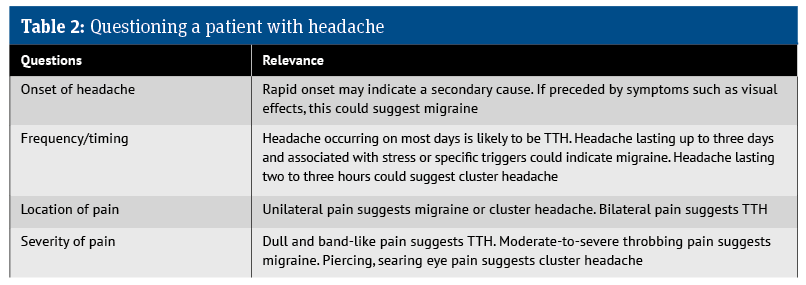
While diagnosing the underlying reason for a headache can be difficult, pharmacists need to be aware of the signs and symptoms associated with the more common causes, as well as any red flags warranting prompt onward referral.
A headache is a pain or throbbing sensation in the head or face, with an estimated lifetime prevalence of over 90%. Most patients self-manage their headaches with OTC analgesics. However, when a headache lasts for an extended period, patients often become concerned that it has a more sinister cause, such as a brain tumour.
Fortunately, most headaches are not caused by brain tumours. Nevertheless, according to the Brain Tumour Charity, up to 60% of people living with a brain tumour develop a headache at some point. Any headache associated with a brain tumour will have specific symptoms, which include:
- Worse in the morning
- Aggravated by activities such as straining, coughing, shouting or bending over
- Pain relieved on standing upright
- Fails to respond to analgesics.
According to the International Headache Society, headaches are categorised as either primary or secondary, with the latter having a clear and identifiable cause, such as a ruptured aneurysm or injury.
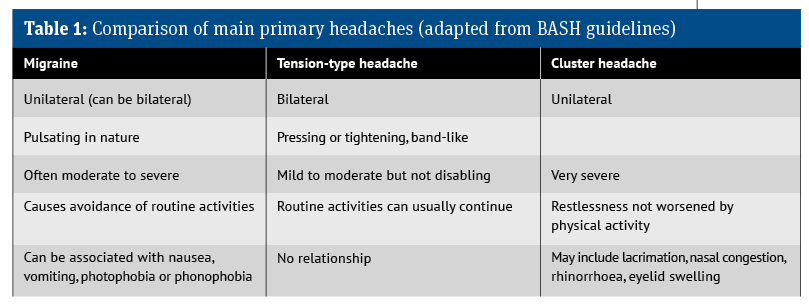
Primary headache is the most common form, accounting for over 90% of cases. There are three main types of primary headache: tension-type headache, migraine and trigeminal autonomic cephalalgia (cluster headache). Pharmacy teams are likely to encounter patients with both tension-type headache and migraine, although they also need to be aware of symptoms suggestive of cluster headache.
Tension-type headache
Tension-type headache (TTH) is by far the most common type of primary headache, with one study estimating a global prevalence of 42%. TTH is subdivided into three categories:
- Infrequent (occurring less than once a month)
- Frequent (at least 10 episodes on fewer than 15 days a month)
- Chronic (more than 15 episodes a month).
Symptoms
Typical presentation is a headache with gradual onset that persists for variable periods, from half an hour to several days, with a constant level of pain – sometimes described as a dull ache. Patients with TTH will classically describe the following symptoms:
- A band of mild-to-moderate bilateral pain
- A sensation of pressing or tightening, like having a tight band around the head
- A headache that is not aggravated by routine physical activity.
There are several possible underlying causes of TTH. Common reasons include:
- Stress, anxiety or lack of sleep
- Eye strain
- Hunger
- Exposure to bright sunlight, heat, cold or noise
- Alcohol, caffeine or dehydration.
Management
Although TTH can last for several days, it is not serious and is generally self-limiting. Consequently, reassurance may be sufficient for most patients. Acute TTH frequently responds well to simple analgesics, such as paracetamol or non-steroidal anti-inflammatory drugs (NSAIDs) including ibuprofen, naproxen or aspirin.
Pregnant and breastfeeding women should use paracetamol. While NSAIDs should be avoided during pregnancy, they can be used during breastfeeding.
Where simple analgesics are ineffective, combination products containing caffeine can be used. Caffeine itself is not effective for acute TTH, but it appears to be beneficial when combined with paracetamol, aspirin or ibuprofen. Opioid drugs should be avoided due to the risk of medication-overuse headache (see below).
When combination therapy fails to provide relief, or when the headaches become chronic, patients should be referred to their GP. Low-dose amitriptyline (10-25mg daily) taken in the evening can help. The dose can then be increased, if tolerated, to a usual dose of 25-75mg daily.
Migraine
Migraine is a chronic/episodic, neurological disorder and the most debilitating form of primary headache. According to an NHS RightCare report in 2019, there are approximately 10 million people in the UK living with migraine.
Migraine can be further divided into two subtypes:
- Migraine without aura
- Migraine with aura (sometimes referred to as ‘classic’ migraine).
Migraines are described as either episodic (occurring on fewer than 15 days a month) or chronic (occurring on more than 15 days a month and persisting for over three months).
A typical sufferer will experience one to two attacks a month. Migraines are two to three times more common in women and around 8% of sufferers have the chronic type.
The precise cause of migraine remains unclear, but is probably due to a combination of genetic, environmental and neurological factors. Between 20-60% of migraine sufferers experience what is termed an intuitive or prodromal phase, sometimes occurring 24-48 hours before symptom onset.
Frequently reported migraine triggers include:
- Stress (most common)
- Disturbed sleep
- Irregular eating or skipping meals
- Excessive caffeine intake
- Dehydration
- Lack of exercise
- Strong odours
- Menstruation.
Diagnosis: migraine without aura
A diagnosis of migraine without aura is based on the following criteria:
- A headache lasting 4-72 hours if untreated or unsuccessfully treated.
AND at least two of the following characteristics:
- Unilateral pain (although in 30-40% of cases, the headache is bilateral)
- Pulsating or throbbing pain
- Moderate-to-severe intensity
- Worsening with physical activity such as walking or climbing stairs.
There should also be at least one of the following:
- Nausea and/or vomiting
- Photophobia or phonophobia.
Migraine with aura
Around a third of patients experience an aura with their migraine. However, a formal diagnosis of migraine with aura still requires patients to fulfil the criteria for migraine without aura, together with aura symptoms.
Aura symptoms are highly variable, although they are characteristically progressive and can occur within an hour before headache onset. Patients may describe seeing zigzag lines, blind spots or changes in vision. Sufferers might also develop unilateral sensory symptoms, such as numbness in one hand or on one side of the face. As mentioned, these symptoms can precede the headache itself by up to 60 minutes.
Management
In the first instance, patients should be advised to avoid recognised migraine triggers wherever possible. It can be helpful to suggest that patients keep an ‘attack and trigger’ diary when attacks are frequent, as this may identify opportunities for behaviour modification. The diary can help determine whether triggers and attacks coincide.
Drug therapy for acute attacks
Simple single-dose analgesics taken at the start of a migraine attack will often suffice, for example:
- Ibuprofen 400mg (if ineffective, consider increasing to 600mg)
- Soluble aspirin 900mg
- Paracetamol 1,000mg where NSAIDs are contraindicated (also suitable during pregnancy).
As with tension-type headaches, opioids should be avoided due to the risk of medication-overuse headache.
Combination therapy
A trial of combination products containing aspirin, paracetamol and caffeine can be effective. A 2022 meta-analysis of seven trials involving 3,306 patients found that this combination provided a clinically relevant response within two hours.
Nausea and vomiting
Patients with nausea or vomiting can be prescribed:
- Metoclopramide or prochlorperazine 5-10mg (or 3mg buccal tablets) every 6-8 hours
- Where vomiting restricts the use of oral agents, intranasal triptans can be used.
If these initial approaches fail to provide relief within two hours, the treatment is unlikely to be effective.
Triptans
Oral triptans, such as sumatriptan 50-100mg, can be taken alone or in combination with either paracetamol or NSAIDs. Furthermore, according to SIGN, sumatriptan 100mg provides superior pain relief compared with aspirin 900mg and paracetamol 1,000mg when combined with metoclopramide.
For patients experiencing aura, sumatriptan should be taken at the onset of the headache, not the aura.
Pregnancy and breastfeeding
For pregnant and breastfeeding women, paracetamol is the preferred first-line treatment for acute episodes, although sumatriptan can also be used. Aspirin should be avoided.
Pregnant women experiencing nausea or vomiting can use both metoclopramide (although not during breastfeeding) and prochlorperazine short-term. Prochlorperazine can also be used short-term during breastfeeding, although use of buccal prochlorperazine during pregnancy and breastfeeding is not usually advised.
Calcitonin gene-related peptide inhibitors
During a migraine attack, activation of the trigeminovascular system leads to an increased release of calcitonin gene-related peptide (CGRP), which, in turn, increases the sensitivity of trigeminal nociceptors. This action causes cerebral vasodilation and transmission of pain signals, leading to the intracranial pain seen in migraine.
The ‘gepants’ are a new class of drugs that inhibit the action of CGRP and were specifically developed for the prophylactic management of migraine. Although NICE has recommended two oral gepants, rimegepant and atogepant, as preventative therapy for episodic migraine, SIGN states that:
- Rimegepant can be used for patients with acute migraine who have had an inadequate response or poor tolerability to two or more triptans, and where paracetamol or NSAIDs have been considered ineffective or unsuitable
- Rimegepant can also be considered for acute migraine where patients have a contraindication to triptans, such as previous myocardial infarction or ischaemic heart disease.
Prophylactic therapy
The decision to initiate prophylactic therapy is recommended where:
- Migraine attacks significantly interfere with a patient’s daily activities despite acute treatment
- Attacks are frequent (on average, more than once a week)
- Acute therapy is either contraindicated or ineffective
- Patients are at risk of medication-overuse headache (see below).
Pharmacotherapy
- Propranolol 80-160mg daily (in divided doses) for episodic or chronic migraine
- Amitriptyline 25-150mg at night
- Atogepant 60mg daily or rimegepant 75mg daily or alternate days (avoid both during pregnancy and breastfeeding)
- Topiramate 50-100mg daily
- Candesartan 16mg daily (unlicensed use) – avoid during pregnancy and breastfeeding.
Although it is a well-established therapy, there is little convincing evidence to recommend pizotifen as a prophylactic treatment.
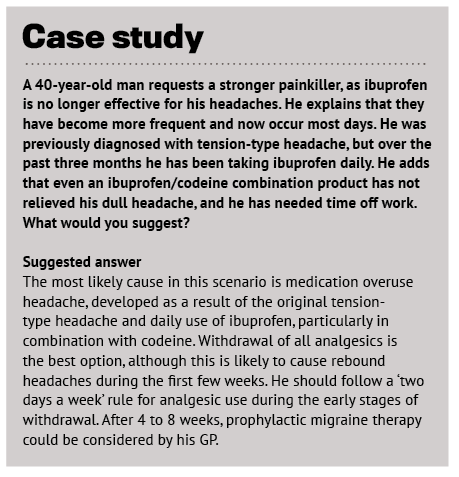
Medication-overuse headache
Pharmacists treating patients with primary headaches need to be mindful of the risk of medication-overuse headache (MOH). This is defined as a headache present on 15 or more days a month in those with a pre-existing primary headache disorder.
In essence, it is a rebound headache that develops because of regular use of one or more drugs – particularly codeine-containing analgesics or triptans – for symptomatic treatment of acute headaches for longer than three months. MOH is most seen in patients with migraine, with one analysis finding it present in 15% of sufferers.
Management
The best approach remains unclear, although common strategies include:
- Abrupt withdrawal of analgesics
- Abrupt withdrawal combined with prophylaxis.
Complete withdrawal of all analgesics is often recommended, but patients should be advised that their headaches are likely to worsen for the first one or two weeks. In addition, patients may experience nausea, vomiting, reduced appetite, tachycardia, sleep disturbance, anxiety and restlessness.
Cluster headache
Cluster headaches are the most common type of trigeminal autonomic cephalalgia, with a lifetime prevalence of roughly 0.12%. The majority (80%) of those affected have the episodic form, while the remainder have a chronic form of the condition.
The headache itself is characterised by attacks (the cluster period) of severe unilateral pain localised to the orbital, peri-orbital and/or temporal areas. Patients often describe the pain as severe and burning, as though they have a hot poker in the eye.
These attacks can last 15-180 minutes and occur from once every other day to as often as eight times a day for up to three months, followed by a period of remission. Triggers include alcohol, strong smells, stress and bright sunlight.
Key associated symptoms
- Eyelid oedema with redness
- Lacrimation
- Nasal congestion/rhinorrhoea
- Agitation.
Management
Patients should be referred to their GP. Acute attacks are managed with subcutaneous sumatriptan and oxygen, while first-line preventative therapy is verapamil.
Secondary headache
A secondary headache arises from another condition, including:
- Sinusitis – dull pain behind the eyes, cheekbones or forehead
- Dehydration – dull ache (although it can be sharp or stabbing) affecting the whole or part of the head, resolving with adequate hydration
- Exercise – throbbing or pounding pain starting either during exercise or after stopping
- Altitude – the most common symptom of altitude sickness when 2,500m above sea level.
Red flags
Red flags associated with headache include:
- A sudden-onset headache that becomes worse within five minutes, also known as a thunderclap headache
- Associated neurological symptoms, such as limb weakness, facial weakness or numbness
- Associated systemic upset, including malaise, fever or fatigue
- Headache in patients aged over 50 years, as this is an independent risk factor for intracranial pathology.