
In Clinical
Follow this topic
Bookmark
Record learning outcomes
Acute otitis media is one of the conditions that comes under the Pharmacy First service, so it is important for pharmacists to know how to diagnose and treat it, and what complications to look out for.
Presentation
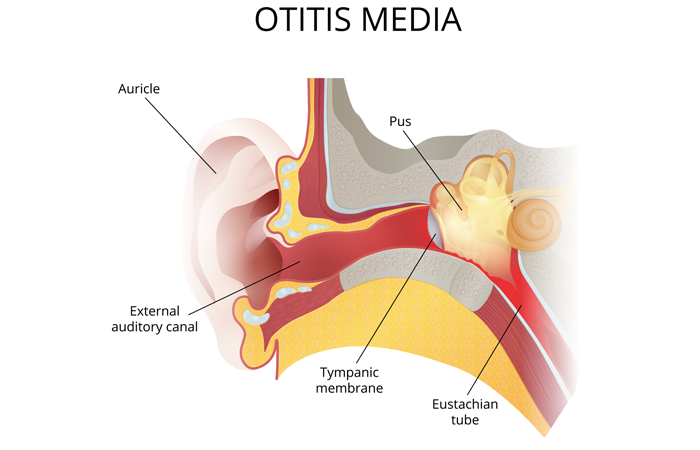
NICE defines acute otitis media as “the presence of inflammation in the middle ear, associated with an effusion and accompanied by the rapid onset of symptoms and signs of an ear infection”.
The condition occurs frequently in children but is less common in adults. It often starts after a cold or sore throat.
According to Kenny Chan, lead information services pharmacist at Numark, acute otitis media can be quite uncomfortable and distressing for sufferers, especially if they are not sure what is going on. “It can appear as a sudden onset of pain, which can be sharp or throbbing,” he says.
“This pain is often accompanied by a feeling of fullness or pressure in the ear. The patient might also experience difficulty hearing – as if sounds are muffled or distant. In some cases, there may be fluid discharging from the ear, which can be a sign of infection.”
Children might show additional symptoms such as irritability, crying more than usual, poor feeding, restlessness, runny nose, cough or have difficulty sleeping. They might also pull at their ears in an attempt to relieve their discomfort.
“It is important to pay attention to these symptoms, as untreated acute otitis media can lead to complications,” says Chan. “The Pharmacy First service allows pharmacies to provide guidance and treatment options to help alleviate the pain and prevent further issues.”
Examination
Under Pharmacy First, with acute otitis media, children and adolescents aged 1-17 years can be seen on a walk-in basis at the pharmacy, or referred to the pharmacy by their GP.
In order to be able to conduct an otitis media consultation, face-to-face training on how to use an otoscope is essential. “I can’t stress enough the importance of knowing how to use an otoscope correctly,” says Lila Thakerar, superintendent pharmacist at Shaftesbury Pharmacy in Harrow. “It is never too late to update your knowledge.”
During the consultation, the otoscope should be gently inserted into the ear to look for signs of infection, such as redness, swelling or fluid behind the eardrum. “These indicators can help determine if acute otitis media is present,” says Chan. “The process is quick and painless, although some pressure may be felt when the otoscope is positioned.”
Diagnosis
Pharmacy First has a diagnostic and treatment framework that must be followed, and each consultation should be person-centred, says Ade Williams, superintendent pharmacist at Bedminster Pharmacy in Bristol. “It is important that when you do have the consultation, you ask questions to make sure your interpretation of what you are seeing is aligned to the patient’s experience,” he says.
Signs to look out for during diagnosis are red, yellow or cloudy membranes, severe bulging of the tympanic membrane, and apparent sticky discharge, says Thakerar.
It is also important to check for any possible complications from pre-existing conditions, such as if the patient has cardiovascular, lung, liver or immunosuppression issues. “While carrying out a diagnosis of acute otitis media, you need to be careful that all the background checks are done,” Thakerar adds.
Red flags include a perforated eardrum and any abnormal growths or changes in the standard features of the inner ear, says Williams.
Treatment
Once acute otitis media has been diagnosed, the most appropriate treatment plan, tailored to the specific needs of the patient, should be discussed.
Pain relief is often a priority, and medications such as paracetamol or ibuprofen can help to alleviate discomfort and reduce fever. “These can be a great first step in managing symptoms while the body fights the infection,” says Chan.
If required, phenazone and lidocaine ear drops can be supplied. A course of antibiotics may also be given via a PGD – after taking a patient history, including whether they have any allergies or intolerances.
When antibiotics are supplied, patients should be reminded to take the full course. “Part of antibiotic stewardship is making sure we are explaining to people what is the right treatment, and why it is the right treatment,” says Williams.
“Sometimes, just monitoring the symptoms is enough, and many ear infections get better on their own within three to five days,” says Alwyn Fortune, policy lead for Royal Pharmaceutical Society (RPS) Wales. “However, if a child’s symptoms have not improved within two to three days, they should be seen by an appropriate healthcare professional.”
While pharmacists are not able to supply treatments for acute otitis media for patients over the age of 17 years under the Pharmacy First service, a minor illness consultation may be carried out if an older patient has been referred to the pharmacy by a GP, says Thakerar.
Making a success of Pharmacy First
The Pharmacy First acute otitis media service seems to be “really relieving the burden across primary care”, says Ade Williams of Bedminster Pharmacy in Bristol. His experience is that it is popular with patients as well as with clinicians.
When patients have earache, Williams says they want to see somebody who is going to have some diagnostic input and guidance for them. Before Pharmacy First, that meant heading to their GP or to urgent care. “It is the examination, it is the management, it is the alleviating of concerns and fears, but also the timely clinical intervention. It is a win for everybody,” he says.
A PGD that covers otitis externa enables the Bedminster team to treat older patients who do not fall within the Pharmacy First criteria.
Nevertheless, Williams believes there should be a “population-wide service” covering acute otitis media and otitis externa in all patient groups. “There is a lot of unmet need and anxiety in the wider population”, he says.
In the meantime, it is important to promote the Pharmacy First service.
“Keep updating GPs that you are able to diagnose and treat patients with acute otitis media under Pharmacy First, and encourage them to refer patients, to free up their time for urgent appointments,” says Lila Thakerar of Shaftesbury Pharmacy in Harrow.
Pharmacies offering earwax microsuction should also make sure this is well publicised. “Tell GPs you are providing the service and ask them to refer patients,” Thakerar advises.
Complications
Dealing with acute otitis media can be quite challenging, says Chan. While most cases resolve without issue, he stresses the importance of being aware of potential complications. This includes the persistence of fluid in the middle ear – known as otitis media with effusion or ‘glue ear’.
“This can lead to temporary hearing loss, which might affect speech and language development in children,” he says. “It is important to monitor people who notice hearing difficulties as they may need the fluid draining.”
Another concern is the spread of infection to nearby structures, such as the mastoid bone behind the ear, which can lead to mastoiditis. “Symptoms might include swelling, redness and tenderness behind the ear. If you suspect mastoiditis, refer to the GP, as it may require antibiotics or, in severe cases, surgical intervention,” says Chan.
In rare instances, untreated infections can lead to more serious complications like meningitis or brain abscess. Symptoms such as severe headache, neck stiffness or changes in consciousness need immediate referral to A&E.
Prevention advice
Pharmacists can help patients avoid problems in the future by passing on appropriate advice, such as the importance of practising good ear hygiene. “This includes keeping ears dry, especially after swimming or showering, by drying them properly,” says Chan.
“Also, with activities such as swimming, earplugs are a very efficient way to keep water out of the ear canal. Avoid inserting objects into the ear. Cotton swabs or other objects should not be used to clean the ear canal as this can push wax further in and potentially cause damage to the eardrum.”
For those experiencing repeated episodes of otitis media, additional preventative measures can be discussed. “This might include lifestyle changes, vaccinations or surgical options to reduce the frequency of infections,” says Chan.
Other common ear conditions
Otitis externa (outer ear infection) is caused by inflammation of the external ear canal.
It is slightly more common in women and is often seen between the ages of 45 and 75 years. It can be caused by a bacterial or fungal infection, an allergy or irritation, such as getting water in the ear while swimming. Damage to the ear canal, wearing hearing aids or eczema can increase the risk. Symptoms include pain, itching, discharge, reduced hearing, tenderness when the ear or jaw are moved, swollen and sore glands in the throat, and a full feeling in the ears.
An OTC acetic acid ear spray can treat mild symptoms in those aged 12 years and over. More severe symptoms may need prescribed antibiotic drops or sprays with or without a corticosteroid.
Vertigo
This is usually symptomatic of a problem with the inner ear caused by an infection (labyrinthitis), migraine or certain medicines. Benign paroxysmal positional vertigo (BPPV) is caused by certain head movements. Ménière’s disease is a rare inner ear condition that can cause vertigo, tinnitus and a loss of hearing. Vertigo often gets better without treatment, although antibiotics may be prescribed if it is caused by an infection, while prochlorperazine or antihistamines may aid balance. Specific exercises can help to improve balance in BPPV.
Excess earwax
Earwax can be removed with OTC ear drops or sprays, or with microsuction, which uses a suction device to remove wax without water. This is now being offered by a growing number of pharmacies. “The procedure requires specialised equipment and expertise to be performed safely,” says Kenny Chan.
During a consultation, discussing ear-related issues such as previous surgeries, infections and conditions like tinnitus helps to tailor the procedure to the patient and avoid complications.
After microsuction, the advice is to avoid cleaning the ears excessively. “The ears will naturally produce wax, and over-cleaning can lead to irritation or infection,” says Chan.
Customers should always be advised not to use cotton buds or other objects to remove earwax.
Further reading
Resources and further reading references for hearing loss, earwax and microsuction can be found in this month’s CPD module.