
In Clinical
Follow this topic
Bookmark
Record learning outcomes
Key facts
|
Acne vulgaris (or simply acne) is a common, chronic inflammatory skin condition affecting around 80% of teenagers (aged 13 to 18 years). Though often perceived as just a teenage problem, acne can persist into adult life, with roughly 26% of women and 12% of men aged 40 to 49 still affected.
Acne can exert a profound and negative psychological impact on sufferers, who might become either self-conscious or embarrassed. What’s more, there is some evidence that those affected by acne believe that their condition is often trivialised by healthcare professionals.
Underlying cause
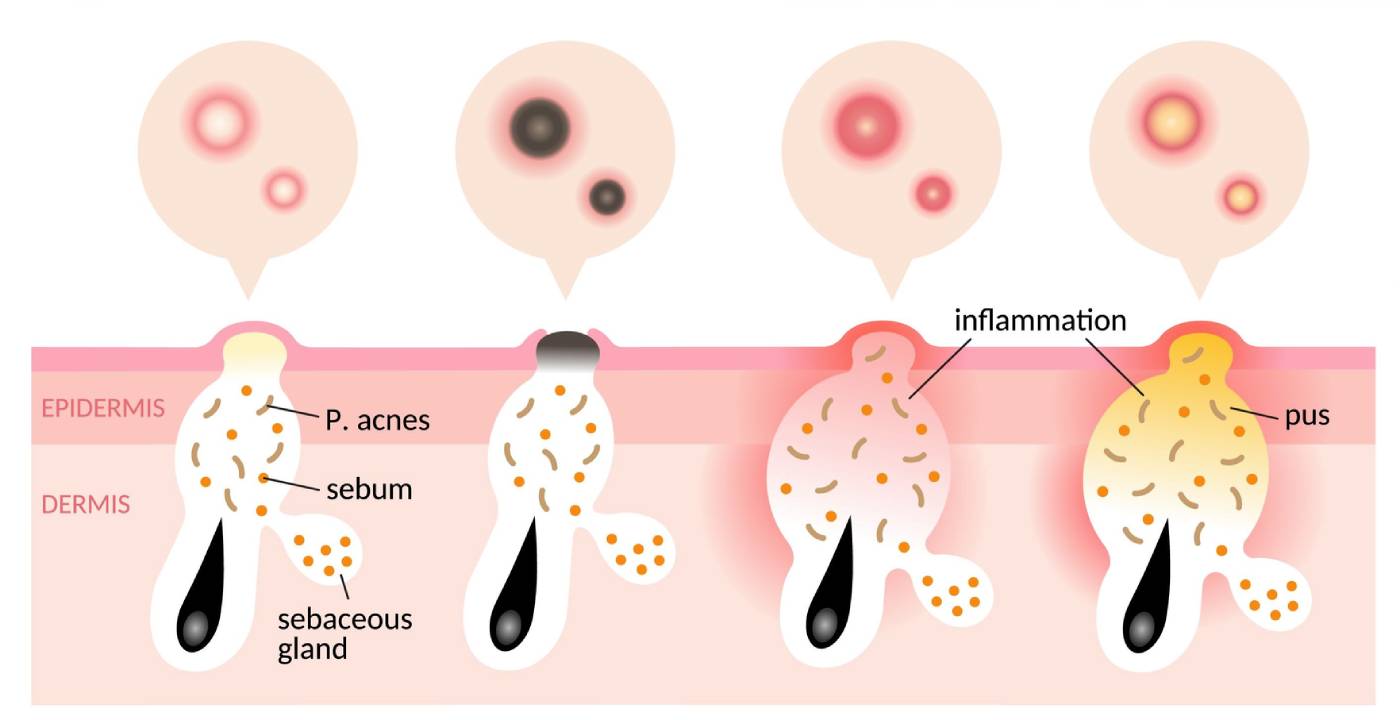
Acne is a disease of the pilosebaceous follicle (see Figure 1 below), which consists of a hair follicle and an associated sebaceous gland. These follicles are much more concentrated in certain areas of the such as the T-zone of the face (forehead and cheeks), the chest, and the back. Consequently, it is these areas that are most commonly affected by acne.
The earliest sign of acne is increased sebum production, which gives the skin a greasy appearance and results from androgen-mediated hyperplasia of the sebaceous glands. Normally, the epithelial keratinocytes lining the pilosebaceous follicle are shed and float in sebum to the skin surface and are washed away.
However, following this increased sebum output in acne, the keratinocytes become unusually cohesive, clumping together, and blocking sebum outflow. This blocked follicle, called a microcomedone, is the initial acne lesion from which all other acne lesions develop. Once a microcomedone is formed, C. acnes an anaerobic, commensal organism within these follicles, thrives in the oxygen-deficient, sealed environment, hydrolysing sebum into glycerol and free fatty acids.
These acids are released into the surrounding epidermis, provoking an immune response that further inflames the skin.
Comedones
Blockages near the skin surface distend the follicular orifice, and melanin, present within desquamated keratinocytes, reacts with the atmosphere, turning black. This produces an open comedone or, more colloquially, a blackhead.
In contrast, if the blockage occurs further down the canal lumen, the increased pressure from sebum trying to escape raises the skin, producing a flesh-coloured lump known as a closed comedone or whitehead. This leads to comedonal acne (see Figure 2 below).

These non-inflamed comedones subsequently develop into papules — small, pink/red, inflamed lesions that can be tender to the touch — and later into pustules (inflamed papules with a white/yellow pus-filled top as illustrated in Figure 1).
More severe acne is characterised by numerous inflammatory lesions, as well as large, solid, painful nodules deep within the skin and cysts, nodules filled with pus. Both nodules and cysts can lead to scarring.
Management
The rationale for treating acne is to reduce the risk of scar formation. Unfortunately, once scars have formed, they are more difficult to treat. Moreover, the NHS does not currently provide treatment for acne scars.
The choice of therapy in acne is severity-dependent, so assessing the extent of a patient’s acne is important. NICE has defined acne severity as follows:
- Mild acne — mostly non-inflamed lesions with a few inflammatory lesions
- Moderate acne — more widespread lesions with a greater number of inflammatory papules and pustules
- Severe acne— widespread inflammatory papules, pustules with nodules or cysts. Scarring may be present.
Where acne affects the chest and back, unless it is mild, referral to the GP is advisable since treatment of these areas with topical agents is more difficult.
Treatment options
Mild to moderate acne is amenable to treatment with OTC products from pharmacy.
Benzoyl peroxide (BPO)
The most effective acne treatment is benzoyl peroxide (BPO), which targets two key pathological processes in acne. It is comedolytic and bactericidal, eliminating C. acnes.
Once in the skin, BPO degrades and releases free-radical oxygen species that oxidise bacterial proteins and physically destroy C. acnes. Given this mode of action, C. acnes cannot develop resistance to BPO, and it remains an effective treatment for mild to moderate acne.
Whilst effective, BPO is also a powerful bleaching agent. It can easily materials (e.g. clothes, pillows, bedding), so patients need to be warned about this before use.
The formulation choice depends on a patient’s skin type. Creams (e.g. Brevoxyl) are appropriate for those with sensitive or dry skin, whereas a gel (e.g. Acnecide), which has a drying effect, is better for greasy skin. Currently, Acnecide is available either as a gel or a gel wash. The gel wash is not a traditional wash product; it is applied to the skin and washed off after two minutes.
Nicotinamide
This vitamin B3 derivative has an anti-inflammatory effect and may be useful for inflamed acne, although it can also reduce sebum excretion. In addition, topical nicotinamide helps to protect the skin barrier against infection and may have a bacteriostatic effect on C. Acnes. Limited evidence suggests that the anti-acne efficacy of nicotinamide is comparable to that of the topical antibiotic clindamycin.
Salicylic acid/facial washes
Salicylic acid has a keratolytic action and is therefore mildly comedolytic (i.e. it breaks down open and closed comedones). A 2% salicylic acid gel formulation is available over the counter to treat acne.
However, NICE does not recommend salicylic acid, perhaps as there is limited evidence of safety and efficacy, although the British Association of Dermatologists suggests it is a first line treatment option. Many facial washes contain lower concentrations of salicylic acid and thus are less effective.
POM treatments
Topical retinoids
Topical retinoids, including adapalene, tazarotene, and tretinoin, are used to treat both noninflammatory and inflammatory acne. These agents normalise follicular keratinisation, reduce keratinocyte cohesiveness, and thereby follicular occlusion and ultimately comedone formation.
NICE recommends a combination of a topical retinoid with BPO as an option for all patients with acne. This combination is complementary, targeting three of the four pathological factors in acne: follicular plugging, inflammation, and a bactericidal effect against C. Acnes.
Furthermore, the comedolytic action of retinoids enhances BPO penetration into the pilosebaceous follicles. One combined fixed-dose retinoid-BPO combination is Epi-Duo.
Azelaic acid
This topical agent exerts bacteriostatic activity against C. Acnes, normalises keratinisation (reducing comedone formation), and reduces inflammation. For people with moderate to severe to acne, NICE recommends topical azelaic acid with an oral antibiotic.
Oral antibiotics
For more widespread acne, oral antibiotics (e.g. lymecycline 408 mg or doxycycline 100 mg daily), in combination with a topical retinoid and BPO, or azelaic acid are recommended. However, antibiotic choices should be based on local formularies.
To reduce the risk of antimicrobial resistance, NICE recommends limiting antibiotic courses to 12 weeks. Additionally, clinicians should avoid antibiotic monotherapy and the combination of a topical and oral antibiotic.
Combined oral contraceptives
The primary driver of ovarian androgen secretion is luteinising hormone, which can be suppressed using a combined oral contraceptive (COC).
While these are effective, none of the currently available COCs are approved for the management of acne, although these are commonly prescribed off-licence as an alternative to oral antibiotics.
It is important to note that co-cyprindiol is licensed for treatment of acne and acts as a contraceptive, but it is not recommended solely for contraception.
Skin of colour
While acne is no more common or severe in patients with skin of colour, a major problem is that post-inflammatory hyperpigmentation (see Figure 3 below) can be significant and often persists for months to years.
Post-inflammatory hyperpigmentation results from inflammation or injury that leads to overproduction or abnormal deposition of melanin in the epidermis or dermis, producing pigmented macules. In fact, this hyperpigmentation is often cited as being more troublesome to patients than the acne itself.

Managing acne in skin of colour
Topical retinoids are highly effective in treating acne and can also improve hyperpigmentation due to their anti-inflammatory properties. In addition, both BPO and azelaic acid are helpful.
However, daily use of these agents can cause dryness and irritation, thereby exacerbating hyperpigmentation. As a result, treatments should initially be used for shorter periods or less frequently (e.g. every few days).
Acne advice
Useful information and advice to give people with acne includes:
- Acne responds slowly to treatment — patients should persevere with any therapy for at least 6 weeks before changing treatment if the response is sub-optimal
- Topical treatments should be applied to the entire affected area, not just the lesions, since emerging micro-comedones may not be visible
- Intake of fatty foods, dairy and chocolate is often seen as an acne trigger. In fact, some evidence suggests that low-glycaemic index diets (e.g. fresh fruits and vegetables) and avoiding foods like white bread and cakes can improve acne
- Red and blue light devices may be effective
- Make-up can block the pilosebaceous follicles. Oil-free alternatives are preferable
- Stress and a lack of sleep are common acne triggers
- Advise patients not to pick at or squeeze acne spots, since this increases the risk of scarring
- Over-cleansing the skin is unnecessary as acne is not caused by poor hygiene, despite the presence of blackheads. Washing twice daily with a non-alkaline or slightly acidic detergent is sufficient.
Managing irritation and dryness
Many topical agents cause skin irritation and dryness. These adverse effects can be managed in one of two ways.
Short-contact therapy
This approach involves applying a retinoid or BPO to the skin for 30-60 minutes, then washing it off. The duration of application can be increased as the skin becomes more tolerant.
However, even when irritation persists, both BPO and retinoids can be used several times per week rather than daily. A pea-sized amount is sufficient; applying larger amounts does not increase efficacy but is likely to increase adverse effects.
Emollient use
Skin dryness can be managed with an emollient. Several emollient ingredients are comedogenic, including isopropyl isostearate, isopropyl myristate, myristyl myristate, coconut butter/oil, and isopropyl palmitate. It might be worth considering an alternative product for people with acne.
Emollients can be applied after either BPO or a retinoid. Patients can continue to use their preferred emollient throughout the day if dryness persists.